Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 65-year-old Caucasian female (CF) is referred by her hematologist and primary care physician (PCP) for work-up of suspected immunodeficiency. She was referred to hematology by her PCP for work-up of frequent urinary tract infections (UTIs) for the last year. Complete blood count with differential (CBCD), bone marrow and chromosomal analysis were negative. Serum immunoglobulins showed low levels of IgG 515 mg/dL (reference range 700 to 1600), IgM 30 (reference range 40 to 230) , IgA 50 (reference range 70 to 400). UA: bacteriuria, no protein. ANA was negative.
Physical examination
Normal.
What is the reason for the low levels of immunoglobulins?
Differential diagnosis:
1. Immunoglobulin loss from GI tract, for example, protein-losing enteropathy. These patients usually have diarrhea but our patient complains of constipation.
2. Immunoglobulin loss in the urine, for example, nephrotic syndrome. IgM (pentamer) and IgA (dimer) are larger molecules than IgG. It is very unlikely to see low levels for IgM in patients with nephrotic syndrome or protein-losing enteropathy. IgG gets filtered in the urine but the large IgM pentamer does not. A 24-hour urine collection is the best method to determine the amount of protein in the urine.
3. Low production of Ig due to bone marrow process or CLL. Both were excluded by BM biopsy and normal CBCD.
4. Common variable immunodeficiency (CVID)
Common variable immunodeficiency (CVID) is the most likely diagnosis in this patient.
How do you diagnose CVID?
A patient with suspected CVID can be tested for the ability to mount humoral and cellular immune response as follows:
1. Humoral immune response.
Inject patient with Pneumovax 23 (not Prevnar, which is a 7-valent conjugate vaccine). Check anti-polysaccharide IgG antibody to pneumococcus serotypes in 3 weeks. There should be a 3-5 fold increase in the anitbody titer to at least 50% of isotypes.
Which serotypes should be included in the order for Ig?
The same serotypes that were included in the given vaccine. Check the enclosed leaflet for this information. For example, the serotypes included in Pneumovax 23 can be found from the Merck website (PDF):
1 2 3 4 5 6B 7F 8 9N 9V 10A 11A 12F 14 15B 17F 18C 19F 19A 20 22F 23F 33F
How to collect the serum for anti-polysaccharide IgG antibodies?
Collect the serum prior to immunization with Pneumovax 23. Store the pre-immunization serum in the office refrigerator. Give the vaccine. Check the post-immunization serum 3 weeks later. Send both pre- and post-immunization serums to the laboratory at the same time.
The pneumococcal vaccine comprises purified capsular polysaccharide of 23 stereotypes that account for more than 90% of the invasive pneumococcal infections in the USA. It induces anti-polysaccharide IgG antibody levels to most or all of the component polysaccharide antigens in immunocompetent adults. Elderly adults respond equally well to vaccination as do younger adults. The current 23-valent vaccine comprises 25 μg of each of 23 pneumococcal stereotypes (namely, serotypes 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F and 33F).
The test should be ordered as follows: Pre- and post-IgM and IgG antibody titers to pneumococcal serotypes 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F and 33F
2. Cellular immune response.
Some patients with CVID have decreased cellular immunity as well. Cellular immunity is tested by anergy panel with common antigens to which the patient was likely exposed in the past: Tetanus toxoid, Trichophyton, Candida. An intradermal injection of 0.1 mL of each antigen is necessary to perform the test. The test is read in 48-72 hours. A positive test result indicates intact delayed-type hypersensitivity. A negative test result to all antigens suggests impaired type IV immunity.
Flow cytometry should also be ordered. Lymphocyte proliferation is a more sensitive test to evaluate cellular immune response.
Delayed-type hypersensitivity (DTH) response
The standardized DTH test includes Candida, tetanus, mumps, and TB. Trichophyton is also commonly used. However, the only FDA-approved reagents for DTH are PPD, Candida and mumps.
What are the normal serum immunoglobulin levels (IgG, IgA, IgM)?
Serum levels of IgM, IgG and IgA vary with age, gender and race.
The IgG and IgA concentrations in children show a gradual rise with increasing age. The IgA level is generally about the same in both sexes. Girls typically have higher IgM and IgG levels than boys.
The confidence interval bounded by two standard deviations about the mean excludes 5% of apparently healthy controls.
Elevated IgM, low IgA, low IgG, low IgM, and elevated IgA are the commonest changes observed in apparently healthy humans.
Humoral immunodeficiency is commonly defined as IgG, IgM or IgA level that is two standard deviations (2 SD) below the mean level for IgG, IgM or IgA, respectively, for the particular age group and gender.
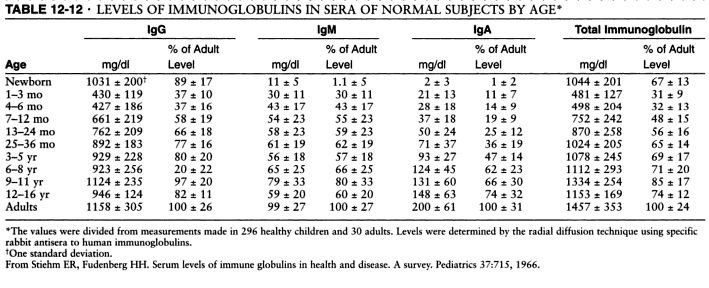
Serum levels of IgM, IgG and IgA. Source: Pediatrics, 1966 and Immunologic disorders in infants and children, by E. Richard Stiehm, Hans D. Ochs, Jerry A. Winkelstein.
Typical pattern of immunoglobulin levels (IgG, IgA, IgM) in humoral immunodeficiency. Click here to enlarge the table.
References
Serum immunoglobulin levels in healthy children and adults. J. W. Stoop, B. J. M. Zegers, P. C. Sander, and R. E. Ballieux. Clin Exp Immunol. 1969 January; 4(1): 101–112.
The relationship of race, sex, and age to concentrations of serum immunoglobulins expressed in international units in healthy adults in the USA. S. E. Maddison, C. C. Stewart, C. E. Farshy, and C. B. Reimer. Bull World Health Organ. 1975; 52(2): 179–185.
Serum immunoglobulin concentrations in preschool children measured by laser nephelometry: reference ranges for IgG, IgA, IgM. D Isaacs, D G Altman, C E Tidmarsh, H B Valman, and A D Webster. J Clin Pathol. 1983 October; 36(10): 1193–1196.
D Isaacs, A D Webster, and H B Valman. Clin Exp Immunol. 1984 November; 58(2): 335–340.
Serum Immunoglobulin Levels Throughout the Life-Span of Healthy Man. Ann of Int Med, November 1, 1971, Vol. 75 no. 5 673-682.
Diagnostic Criteria for Common Variable Immunodeficiency (CVID): Probable and Possible Diagnosis
The diagnostic criteria are divided into three categories: definitive, probable, and possible. There are no criteria for definitive diagnosis of Common Variable Immunodeficiency (CVID) at this time.
To guard against the inclusion of patients who have polymorphic variants in the genes associated with immunodeficiency and to specify the clinical or laboratory finding that is most consistently abnormal in a particular disorder, the patient must fulfill an inclusion criterion that is characteristic of the disorder.
Definitive diagnosis
Patients with a definitive diagnosis are assumed to have a greater than 98% probability that in 20 years they will still be given the same diagnosis. Mutation detection is the most reliable method of making a diagnosis but a single mutation is rarely found in CVID.
Probable diagnosis
Patients with a probable diagnosis are those with all of the clinical and laboratory characteristics of a particular disorder but who do not have a documented abnormality in the gene, the mRNA, or the protein that is known to be abnormal in the disorder. They are assumed to have a greater than 85% probability that in 20 years they will be given the same diagnosis.
Probable diagnosis of CVID:
Male or female patient who has a marked decrease (at least 2 SD below the mean for age) in serum IgG AND IgA and fulfills all of the following criteria:
1. Onset of immunodeficiency at greater than 2 years of age.
2. Absent isohemagglutinins and/or poor response to vaccines.
3. Defined causes of hypogammaglobulinemia have been excluded
Possible diagnosis
Patients with a possible diagnosis are those that have some but not all of the characteristic clinical or laboratory findings of a particular disorder.
Possible diagnosis if CVID:
Male or female patient who has a marked decrease (at least 2 SD below the mean for age) in one of the major isotypes (IgM, IgG, and IgA) and fulfills all of the following criteria:
1. Onset of immunodeficiency at greater than 2 years of age.
2. Absent isohemagglutinins and/or poor response to vaccines.
3. Defined causes of hypogammaglobulinemia have been excluded
Clinical features of CVID
Most patients with CVID are diagnosed with immunodeficiency in the second, third, or fourth decade of life, after they have had several pneumonias; however, children and older adults may be affected.
Viral, fungal, and parasitic infections as well as bacterial infections may be found.
The serum concentration of IgM is normal in about half of the patients.
Abnormalities in T cell numbers or function are common. The majority of patients have normal numbers of B cells; however, some have low or absent B cells.
Approximately 50% of patients have autoimmune manifestations. There is an increased risk of malignancy.
Differential diagnosis of hypogammaglobulinemia includes drug-induced, for example secondary to glucocorticoids (steroids).
References
Diagnostic Criteria for Primary Immunodeficiencies. Mary Ellen Conley, Luigi D. Notarangelo, and Amos Etzioni Representing PAGID (Pan-American Group for Immunodeficiency) and ESID (European Society for Immunodeficiencies). Clinical Immunology, Vol. 93, No. 3, December, pp. 190–197, 1999.
Recognizing Primary Immune Deficiency in Clinical Practice. Clinical and Vaccine Immunology, March 2006, p. 329-332, Vol. 13, No. 3.
What is the treatment for CVID?
Intravenous immunoglobulin (IVIG) administered at outpatient clinic, monthly, this is the most common treatment.
Subcutaneous immunoglobulin G (SCIG), administered at home, given weekly.
Summary
CVID is characterized by:
1. Low levels of most or all of the immunoglobulin (Ig) classes
2. Lack of B lymphocytes or plasma cells that are capable of producing antibodies
3. Frequent bacterial infections
CVID is the most common primary immunodeficiency with an incidence of 1 case per 10,000-50,000 population. More than two thirds of patients are aged 21 years or older when CVID is diagnosed. CVID represents a group of heterogeneous conditions. Approximately 50% of patients with the deficiency also have diminished serum immunoglobulin M (IgM) levels and T-lymphocyte dysfunction. About 20% of those with CVID have an autoimmune disease.
The prognosis for patients with CVID is good if they do not have bronchiectasis, autoimmune disease or malignancy.

Five immunoglobulin classes (mind map)
In order of their serum concentrations:
IgG 1000 mg/dL
IgA 200 mg/dL
IgM 150 mg/dL
IgD 4 mg/dL
IgE 0.005 mg/dL (extremely low serum concentration compared to other Ig in (GAMED)
IgG and A are divided in subclasses: 4 for IgG -- IgG1, IgG2, IgG3, IgG4, and 2 for IgA -- IgA1 and IgA2.

Ig structures. Image source: Wikipedia.
{kind=link}
Can patients with CVID receive live vaccines?
Patients with CVID should never receive live vaccines and should be advised to avoid contact with children or adults who have recently been given a live vaccine, for example, FluMist® nasal flu vaccine spray.
Can patients with CVID travel to endemic area for hepatitis A or B?
Yes but they should be given hyperimmune Ig prior to travel to endemic areas. The hyperimmune Ig provides protection for 3 weeks.
What is the half-life of IVIG?
3 weeks.
Mnemonic: Dose of IVIG in PIDD
400-600 mg/kg/month
4 letter words:
IVIG
CVID
SCID
What are the long-term risks for patients with CVID?
Malignancies, autoimmune diseases, infections.
FDA guidelines for IVIG state the product should be prepared out of at least 1,000 different human donors. Most commercial IVIG preparations contain products from over 10,000 human donors which increases the risk of acquiring diseases such as HIV, HCV or Creutzfeldt-Jakob disease. The risk is small but nevertheless, it should be discussed with the patient.
What HIV screening test would you do in a patient with CVID?
Patients with CVID can not produce an adequate antibody response to the HIV virus if infected and ELISA or Western blot are not useful. PCR RNA is the test of choise for HIV diagnosis in patients with CVID.
Can patients with CVID still have allergies?
Yes, the production of IgE may not be affected in patients with CVID can have symtpoms of allergic rhinitis, urticaria and other IgE-mediated diseases.
Differences between commercial IVIG preparations: Gammagard and Octagam
Gammagard Liquid is the first 10% IVIG solution with no added carbohydrates or sodium. Baxter is replacing Gammagard S/D with Gammagard Liquid.
Sodium concentration
Gammagard: No added sodium. When reconstituted with the total volume of diluent (Sterile Water for Injection, USP) supplied to 5%, Gammagard contains a physiological concentration of sodium chloride (approximately 8.5 mg/mL) and has a pH of 6.8 ± 0.4.
Octagam: sodium content of the final solution is ≤ 30 mmol/l and the pH is between 5.1 and 6.0.
Osmolality
Gammagard osmolality is 240-300 mOsmol/kg, similar to physiological osmolality (285 to 295 mOsmol/kg).
Octagam osmolality is 310 - 380 mosmol/kg.
Cost
Gammagard Liquid, Baxter, $129.60/gm
Octagam, Octapharma, $118.34/gm
References
Antibody response of pneumococcal vaccine: need for booster dosing? International Journal of Antimicrobial Agents, Volume 14, Issue 2, March 2000, Pages 107-112.
How to identify a possible specific antibody deficiency to pneumococcus. AAAAI, 2007.
Common Variable Immunodeficiency. eMedicine.
Common Variable Immunodeficiency. eMedicine.
Common Variable Immunodeficiency: A Multifaceted And Puzzling Disorder. Expert Review of Clinical Immunology, Medscape, 2009.
Primary Immunodeficiency Diseases: Definition, Diagnosis, and Management. Nima Rezaei, Luigi D. Notarangelo, Asghar Aghamohammadi, 2008, Google eBook.
Common variable immunodeficiency (CVID). Allergologia et Immunopathologia. November 2006. Volume 34 - Number 06 p. 263 - 275.
Adaptive Humoral Immunity: B-cells and Immunoglobulins
Mnemonics: Adaptive Humoral Immunity: B-cells and Immunoglobulins
Intravenous immune globulin. Hopkins HIV Guide.
Common variable immunodeficiency (CVID). Allergologia et Immunopathologia. November 2006. Volume 34 - Number 06 p. 263 - 275.
Adaptive Humoral Immunity: B-cells and Immunoglobulins
Mnemonics: Adaptive Humoral Immunity: B-cells and Immunoglobulins
Intravenous immune globulin. Hopkins HIV Guide.
Evaluation and diagnosis of common variable immunodeficiency. UpToDate.
Octagam, Octapharma.
Gammagard Liquid, Baxter.
Octagam, Octapharma.
Gammagard Liquid, Baxter.
Interpretation of pneumococcal antibody titers - AAAAI Ask the Expert, 2011.
Assessment of antibody response to pneumococcus immunization. AAAAI, Ask the Expert, 2011.
Cost-effectiveness of Pneumococcal Conjugate Vaccine vs. Polysaccharide Vaccine in Adults: PCV13 was better than PPSV23. JAMA, 2012.
Cost-effectiveness of Pneumococcal Conjugate Vaccine vs. Polysaccharide Vaccine in Adults: PCV13 was better than PPSV23. JAMA, 2012.
Published: 07/12/2008
Updated: 02/06/2012
7 comments:
Why would you bother with bone marrow and chromosomal analysis? Isn't the vaccine challenge far less invasive and less expensive?
Mark,
Thank you for your comment. CBCD, bone marrow and chromosomal analysis were done by the hematologist prior to the referral to our clinic.
Did you do any B cell markers such as CD19?
If the ANA was positive would CVID still be the diagnosis?
It depends on the sequence. Patients with CVID are at higher risk for developing autoimmune diseases. If the ANA turns positive after CVID is already diagnosed, the diagnosis is still CVID.
Can a 75 year old female with low IgG,IgA,and IgM pass a pneumovax challenge and still have CVID or a PIDD? I have been diagnosed with selective IgM deficiency and a T-cell clonal disorder by several Drs. and just recently had a pneumovax challenge done 5 months after my last IVIG infusion. I have several autoimmune diseases and am being screened for lupus.
I am a 28 year old female. My symptoms are low blood platelets, weight loss of >40lbs in 8 months, bruising for no reason, malabsorption, "allergy" to Tetanus vaccine repeated serious infections and severe fatigue. I have had several tests done including multiple blood tests by a hematologist, stool cultures, and colonoscopy. I have gotten very tired of tests and Drs and have decided to do a little of my own research. That is when is discovered CVID. I feel that a lot of the information that I read applies to me. If i go see an immunologist, what questions should I ask? Does it sound like I have reason to think this may be worth looking into?
Post a Comment