Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 34-year-old female is in the Allergy/Immunology clinic today for a follow-up of Common Variable Immune Deficiency (CVID). She was last seen in the clinic 3 months ago. Since then, her condition has remained stable and the level of immunoglobulin G has been higher than 700. She is receiving IVIG 90 gm IV every month. She is pre-medicated with Tylenol and oral antihistamines and is able to tolerate the infusions well and has not had any infections of the sinuses or lung infections recently. She however reports painful area in her left armpit for the past two weeks, and it looks like she is developing hidradenitis.
Past medical history (PMH)
Common Variable Immune Deficiency (CVID).
Physical examination
The physical examination is positive for induration and erythema in the right axia which was diagnosed as hidradenitis. The rest of her examination is normal.
What is the most likely diagnosis?
This is a patient with CVID which has been stable on the IVIG replacement at the dose of 90 gm of Gammaguard every month. She also has hidradenitis in the left axilla.
What would you do?
Continue Gammaguard at a dose of 90 grams IV every month. Repeat the level in three months. For her hidradenitis, we recommended Keflex 500 mg PO B.I.D. x 7days.
The patient is planning a trip to the Bahamas for a week in the coming month. She wants to know if she should take any antibiotics with her.
What antibiotics would you prescribe, if she needs any?
Regarding her trip to the Bahamas: in case she develops respiratory or gastrointestinal infection we provided her with a prescription for Levaquin 500 PO QD x 7 days. She is to return to the clinic in four months.
What are the normal serum immunoglobulin levels (IgG, IgA, IgM)?
Serum levels of IgM, IgG and IgA vary with age, gender and race.
The IgG and IgA concentrations in children show a gradual rise with increasing age. The IgA level is generally about the same in both sexes. Girls typically have higher IgM and IgG levels than boys.
The confidence interval bounded by two standard deviations about the mean excludes 5% of apparently healthy controls.
Elevated IgM, low IgA, low IgG, low IgM, and elevated IgA are the commonest changes observed in apparently healthy humans.
Humoral immunodeficiency is commonly defined as IgG, IgM or IgA level that is two standard deviations (2 SD) below the mean level for IgG, IgM or IgA, respectively, for the particular age group and gender.
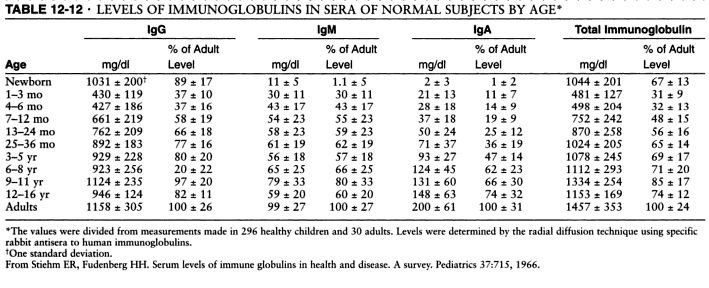
Serum levels of IgM, IgG and IgA. Source: Pediatrics, 1966 and Immunologic disorders in infants and children, by E. Richard Stiehm, Hans D. Ochs, Jerry A. Winkelstein.
Typical pattern of immunoglobulin levels (IgG, IgA, IgM) in humoral immunodeficiency. Click here to enlarge the table.
References
Serum immunoglobulin levels in healthy children and adults. J. W. Stoop, B. J. M. Zegers, P. C. Sander, and R. E. Ballieux. Clin Exp Immunol. 1969 January; 4(1): 101–112.
The relationship of race, sex, and age to concentrations of serum immunoglobulins expressed in international units in healthy adults in the USA. S. E. Maddison, C. C. Stewart, C. E. Farshy, and C. B. Reimer. Bull World Health Organ. 1975; 52(2): 179–185.
Serum immunoglobulin concentrations in preschool children measured by laser nephelometry: reference ranges for IgG, IgA, IgM. D Isaacs, D G Altman, C E Tidmarsh, H B Valman, and A D Webster. J Clin Pathol. 1983 October; 36(10): 1193–1196.
D Isaacs, A D Webster, and H B Valman. Clin Exp Immunol. 1984 November; 58(2): 335–340.
Serum Immunoglobulin Levels Throughout the Life-Span of Healthy Man. Ann of Int Med, November 1, 1971, Vol. 75 no. 5 673-682.
Diagnostic Criteria for Common Variable Immunodeficiency (CVID): Probable and Possible Diagnosis
The diagnostic criteria are divided into three categories: definitive, probable, and possible. There are no criteria for definitive diagnosis of Common Variable Immunodeficiency (CVID) at this time.
To guard against the inclusion of patients who have polymorphic variants in the genes associated with immunodeficiency and to specify the clinical or laboratory finding that is most consistently abnormal in a particular disorder, the patient must fulfill an inclusion criterion that is characteristic of the disorder.
Definitive diagnosis
Patients with a definitive diagnosis are assumed to have a greater than 98% probability that in 20 years they will still be given the same diagnosis. Mutation detection is the most reliable method of making a diagnosis but a single mutation is rarely found in CVID.
Probable diagnosis
Patients with a probable diagnosis are those with all of the clinical and laboratory characteristics of a particular disorder but who do not have a documented abnormality in the gene, the mRNA, or the protein that is known to be abnormal in the disorder. They are assumed to have a greater than 85% probability that in 20 years they will be given the same diagnosis.
Probable diagnosis of CVID:
Male or female patient who has a marked decrease (at least 2 SD below the mean for age) in serum IgG AND IgA and fulfills all of the following criteria:
1. Onset of immunodeficiency at greater than 2 years of age.
2. Absent isohemagglutinins and/or poor response to vaccines.
3. Defined causes of hypogammaglobulinemia have been excluded
Possible diagnosis
Patients with a possible diagnosis are those that have some but not all of the characteristic clinical or laboratory findings of a particular disorder.
Possible diagnosis if CVID:
Male or female patient who has a marked decrease (at least 2 SD below the mean for age) in one of the major isotypes (IgM, IgG, and IgA) and fulfills all of the following criteria:
1. Onset of immunodeficiency at greater than 2 years of age.
2. Absent isohemagglutinins and/or poor response to vaccines.
3. Defined causes of hypogammaglobulinemia have been excluded
Clinical features of CVID
Most patients with CVID are diagnosed with immunodeficiency in the second, third, or fourth decade of life, after they have had several pneumonias; however, children and older adults may be affected.
Viral, fungal, and parasitic infections as well as bacterial infections may be found.
The serum concentration of IgM is normal in about half of the patients.
Abnormalities in T cell numbers or function are common. The majority of patients have normal numbers of B cells; however, some have low or absent B cells.
Approximately 50% of patients have autoimmune manifestations. There is an increased risk of malignancy.
Differential diagnosis of hypogammaglobulinemia includes drug-induced, for example secondary to glucocorticoids (steroids).
References
Diagnostic Criteria for Primary Immunodeficiencies. Mary Ellen Conley, Luigi D. Notarangelo, and Amos Etzioni Representing PAGID (Pan-American Group for Immunodeficiency) and ESID (European Society for Immunodeficiencies). Clinical Immunology, Vol. 93, No. 3, December, pp. 190–197, 1999.
Recognizing Primary Immune Deficiency in Clinical Practice. Clinical and Vaccine Immunology, March 2006, p. 329-332, Vol. 13, No. 3.
Frequency of follow-up visits in a patient receiving intravenous immunoglobulin (IVIG) infusions - every 6 months? AAAAI Ask the Expert, 2011.
Outcome of allogeneic stem cell transplantation (ASCT) in adults with common variable immunodeficiency (CVID) (JACI, 2011).
Frequency of follow-up visits in a patient receiving intravenous immunoglobulin (IVIG) infusions - every 6 months? AAAAI Ask the Expert, 2011.
Outcome of allogeneic stem cell transplantation (ASCT) in adults with common variable immunodeficiency (CVID) (JACI, 2011).
Published: 05/12/2010
Updated: 11/23/2011
No comments:
Post a Comment