Author: V. Dimov, M.D., Allergist/Immunologist, Cleveland Clinic
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU, Fort Lauderdale
A 61-year-old female is in the allergy clinic for evaluation of suspected anaphylaxis. No history of asthma, allergic rhinitis, food allergy, or atopic dermatitis. She had a negative skin and blood tests for multiple food and airborne allergens. The total IgE was low normal at 20. She also had normal normal C-1INH levels (qualitative and quantitative), CBCD, CMP, ANA, and ESR.
She had 4 episodes of symptoms suggestive of anaphylaxis, always during the hot days of the summer, separated about one year apart. All episodes occurred outside with temperatures exceeding 80F. She felt throat discomfort, and teary eyes. During one of the episodes she felt tingling in the last two fingers of the left hand. Three of the episodes were related to consuming wine and salad. There was no significant improvement with epinephrine (EpiPen) use during the last episode. She was found to be slightly hypotensive and tachycardic in the ER after the last episode.
Past Medical History, Past Surgical History: Unremarkable.
Family Medical History: Several members with coronary artery disease (CAD).
Social History: 15-ppd smoking history, quit 2 years ago.
Current Medications: Epinephrine p.r.n.
Drug allergies: Reviewed. NKDA.
Review Of Systems: 12/14 systems were reviewed, negative apart from history of present illness above.
Physical Examination: Unremarkable.
Procedures done today: Spirometry showed FVC 60% and FEV1 61% of predicted, with normal shape of the flow volume curve.
What is the likely diagnosis?
Suspected idiopathic anaphylaxis. No evidence of FDEIA.
Differential diagnosis includes:
- CAD - she has a strong family history and some suggestive symptoms - throat tightness, tingling of the last 2 fingers of the left hand.
- COPD - she has a low FEV1 and a smoking history. No active symptoms.
- syncope symptoms
What would you suggest for management?
The diagnosis of exclusion is suspected idiopathic anaphylaxis - with triggers such as alcohol, heat, exercise (nonimmunological triggers that cause direct activation of mast cells). If tryptase is normal within 3 hours of any future event, anaphylaxis would be unlikely.
There are no symptoms of sulfite hypersensitivity or latex allergy. Food or airborne allergens are not likely to play a significant role (she had both a negative blood and skin test). There was no significant improvement with epinephrine use.
What lab work would you suggest?
Lab work for baseline tryptase level, CH50 and C4 was suggested.
The recommendations include:
- Pulmonary consult for COPD
- Cardiology consult for suspected angina equivalent vs. syncope
- if there are future attacks - obtain tryptase in the ER within 3 hours of the attack along with plasma and urinary histamine (instructions were provided to the patient)
Use epinephrine autoinjector (EpiPen or Auvi-Q 0.3) and call 911 if anaphylaxis develop. A follow-up in 1-3 months was suggested.
Summary
There are 4 broad groups with triggers of anaphylaxis:
1. Allergen triggers (IgE-dependent immunologic mechanism)
Foods, especially peanut, tree nut, shellfish, fish, milk, egg
Insect stings (eg, Hymenoptera venom) and insect bites (eg, kissing bugs, mosquitoes)
Medications (eg, beta-lactam antibiotics, some nonsteroidal antiinflammatory drugs [NSAIDs])
Biological materials, including allergens, allergen immunotherapy, monoclonal antibodies, vaccines to prevent infectious disease, and hormones (eg, progesterone)
Natural rubber latex
Food additives, including spices, insect-derived colorants (eg, carmine), and vegetable gums
Inhalants (rare), eg, horse dander
Human seminal fluid (rare trigger of anaphylaxis in women)
Occupational allergens (eg, stinging insects, natural rubber latex)
2. Immunologic triggers (IgE-independent mechanism)
IgG-dependent (rare) eg, to high molecular weight dextran, infliximab
Coagulation system activation
3. Idiopathic anaphylaxis
Consider the possibility of a hidden or previously unrecognized trigger
Consider the possibility of mastocytosis or a clonal mast cell disorder
4. Nonimmunologic triggers (direct activation of mast cells and basophils)
Physical factors (eg, exercise, cold, heat, sunlight/ultraviolet radiation)
Medications (eg, opioids, some NSAIDs)
Alcohol (ethanol)
Instructions for optimal collection and handling of blood samples for measurement of tryptase and histamine following suspected anaphylaxis
Tryptase (serum or plasma)
When to collect the sample: Blood should be collected between 15 minutes and 3 hours after symptom onset whenever possible; samples collected less 15 minutes or more than 3 hours after symptom onset are less likely to be informative.
How to collect the sample: Blood can be drawn using standard technique. Collect blood for serum (red top tube) or plasma (tube with heparin, citrate or EDTA). A minimum of 1 mL is recommended. For postmortem samples, collect blood from the femoral artery or vein, not the heart.
How to process the sample: Serum or plasma should be placed on ice and frozen as soon as possible. Samples should be shipped frozen by overnight courier if the assay cannot be performed on site.
Histamine (plasma)
When to collect the sample: Plasma for histamine levels should be collected between 5 and 15 minutes after symptom onset; samples collected less than 5 minutes or more than 15 minutes after symptom onset are less likely to be informative.
How to collect the sample: Pull blood manually (DO NOT use vacuum tubes) under gentle pressure through a 20 gauge or larger needle into a syringe containing either citrate or EDTA.
How to process the sample: Anticoagulated blood should be placed on ice and centrifuged to separate plasma from cells as soon as possible, and then the plasma frozen until ready to be analyzed.
The assay for total tryptase is standardized. The assay for histamine is not standardized. Plasma is used to avoid the artifactual release of histamine from basophils that can occur during blood clotting.
Anaphylaxis is common (1 in 20 adults), 50% never received epineprine, the majority have life-threatening reactions. Anaphylaxis represents a huge opportunity for clinical improvement (Wood, JACI, 2014).
References
Anaphylaxis: Confirming the diagnosis and determining the trigger(s). UpToDate, 2013.
Anaphylaxis: Rapid recognition and treatment. UpToDate, 2013.
Published: 08-20-2013
Updated: 09-17-2013
Showing posts with label Anaphylaxis. Show all posts
Showing posts with label Anaphylaxis. Show all posts
Anaphylaxis Action Plan
Editor: V. Dimov, M.D., Allergist/Immunologist, Assistant Professor at University of Chicago
Click here for the Anaphylaxis Action Plan (adapted by Dr. Dimov):
The generic version of the Anaphylaxis Action Plan is available from the AAAAI website (PDF).
References
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011. Full text PDF is available.
Published: 06/07/2011
Updated: 06/11/2012
Click here for the Anaphylaxis Action Plan (adapted by Dr. Dimov):
The generic version of the Anaphylaxis Action Plan is available from the AAAAI website (PDF).
References
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011. Full text PDF is available.
Published: 06/07/2011
Updated: 06/11/2012
How To Use Epinephrine Autoinjector - Auvi-Q or EpiPen
Editor: V. Dimov, M.D., Allergist/Immunologist, Assistant Professor at University of Chicago
This 2-minute video shows the Sanofi's new voice guided Auvi-Q epinephrine injector in action:
Start here: How to use EpiPen. Self-injectable epinephrine (SIE) in the form of a device (EpiPen) was first introduced in 1980.
Video instructions on use of the EpiPen (epinephrine/adrenaline) autoinjector for anaphylaxis from the Australasian Society of Clinical Immunology and Allergy (ASCIA):
How To Use an EpiPen video from Nationwide Children's Hospital in Columbus, Ohio:
Tips for managing food allergy (MJA, 2004):
- Always carry an EpiPen 2-Pak
- Always read food labels
- Ask questions about food preparation (be aware of the risk of cross-contamination)
- No label/no eat
- No EpiPen/no eat
- Tell friends about a serious food allergy
- Tell friends if feeling unwell, especially after eating
The action plans for food allergy and anaphylaxis include the use of EpiPen as first line of treatment.
Key points:
- There is no cure for food allergies at this time
- 8% of U.S. children under 18 have at least one food allergy
- Epinephrine is the first line life-saving medication in severe food allergic reaction. Always carry an EpiPen with you, and remember these simple memory rules in severe food allergic reaction:
- "No Epi, no eat-y" (always carry an EpiPen with you, don't sit down to eat if you don't have an EpiPen available)
- "If it's more than the skin, the Epi goes in" (only mild hives may respond to antihistamine, for anything else you may need an EpiPen)
References
How to use Epipen (official video)
Official EpiPen App for iPhone and iPad
Action plans: asthma, food allergy, rhinitis, anaphylaxis
Training of trainers on epinephrine autoinjector use increases correct use from 23.3% to 74.2% http://goo.gl/lMfSR
Food allergy and anaphylaxis training - free at AllergyReady.com
Time epinephrine needs to reach muscle - holding the device in place for 1 second is as effective as 10 seconds. Annals of Allergy, Asthma and Immunology, 2011.
Related reading
"Epinephrine is to anaphylaxis as an AED (defibrillator) is to someone suffering cardiac arrest. Life-saving." Forbes, 2012.
Published: 01/29/2011
Updated: 05/12/2012
This 2-minute video shows the Sanofi's new voice guided Auvi-Q epinephrine injector in action:
Start here: How to use EpiPen. Self-injectable epinephrine (SIE) in the form of a device (EpiPen) was first introduced in 1980.
Video instructions on use of the EpiPen (epinephrine/adrenaline) autoinjector for anaphylaxis from the Australasian Society of Clinical Immunology and Allergy (ASCIA):
How To Use an EpiPen video from Nationwide Children's Hospital in Columbus, Ohio:
Tips for managing food allergy (MJA, 2004):
- Always carry an EpiPen 2-Pak
- Always read food labels
- Ask questions about food preparation (be aware of the risk of cross-contamination)
- No label/no eat
- No EpiPen/no eat
- Tell friends about a serious food allergy
- Tell friends if feeling unwell, especially after eating
The action plans for food allergy and anaphylaxis include the use of EpiPen as first line of treatment.
Key points:
- There is no cure for food allergies at this time
- 8% of U.S. children under 18 have at least one food allergy
- Epinephrine is the first line life-saving medication in severe food allergic reaction. Always carry an EpiPen with you, and remember these simple memory rules in severe food allergic reaction:
- "No Epi, no eat-y" (always carry an EpiPen with you, don't sit down to eat if you don't have an EpiPen available)
- "If it's more than the skin, the Epi goes in" (only mild hives may respond to antihistamine, for anything else you may need an EpiPen)
References
How to use Epipen (official video)
Official EpiPen App for iPhone and iPad
Action plans: asthma, food allergy, rhinitis, anaphylaxis
Training of trainers on epinephrine autoinjector use increases correct use from 23.3% to 74.2% http://goo.gl/lMfSR
Food allergy and anaphylaxis training - free at AllergyReady.com
Time epinephrine needs to reach muscle - holding the device in place for 1 second is as effective as 10 seconds. Annals of Allergy, Asthma and Immunology, 2011.
Related reading
"Epinephrine is to anaphylaxis as an AED (defibrillator) is to someone suffering cardiac arrest. Life-saving." Forbes, 2012.
Published: 01/29/2011
Updated: 05/12/2012
Food-dependent exercise-induced anaphylaxis (FDEIA)
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Food-dependent exercise-induced anaphylaxis (FDEIA) is a special form of food allergy where a food-intake alone does not induce any symptoms. Anaphylaxis occurs only when triggering factors such as exercise or aspirin-intake are added after ingestion of the causative food.
Clinical features of FDEIA
In FDEIA, patients develop anaphylaxis after eating and exercising. They have no symptoms are rest.
Sequence of events: eating --> exercise --> anaphylaxis
Foods associated with FDEIA
Wheat is the most common food associated with food-dependent exercise-induced anaphylaxis (FDEIA). Both exercise and aspirin-intake facilitate allergen absorption from the gastrointestinal tract.
80% of the patients with wheat-induced FDEIA have IgE reacting to omega-5 gliadin and the remaining of the patients to high molecular weight glutenin (HMW-glutenin).
Which of the following foods is often associated with food-dependent exercise-induced anaphylaxis (FDEIA)?
(A) peanut
(B) fish
(C) wheat
(D) soy
(E) egg
(F) milk
Answer: C.
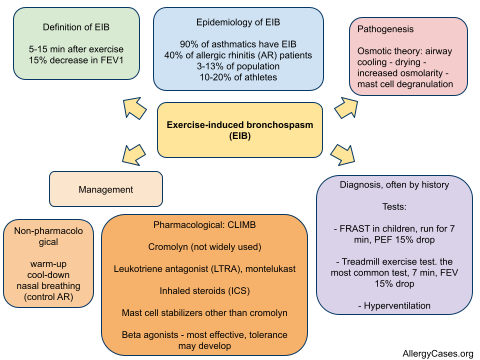
Please note that FDEIA is different from exercise-induced bronchospasm (EIB) (click to enlarge the image):
References
Food-Dependent Exercise-Induced Anaphylaxis-Importance of Omega-5 Gliadin and HMW-Glutenin as Causative Antigens for Wheat-Dependent Exercise-Induced Anaphylaxis. Morita E, Matsuo H, Chinuki Y, Takahashi H, Dahlström J, Tanaka A. Allergol Int. 2009 Oct 25;58(4).
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Food-dependent exercise-induced anaphylaxis (FDEIA) is a special form of food allergy where a food-intake alone does not induce any symptoms. Anaphylaxis occurs only when triggering factors such as exercise or aspirin-intake are added after ingestion of the causative food.
Clinical features of FDEIA
In FDEIA, patients develop anaphylaxis after eating and exercising. They have no symptoms are rest.
Sequence of events: eating --> exercise --> anaphylaxis
There are two types of patients with food-dependent EIA ("generalists" and "specialists"):
- Patients who develop anaphylaxis when exercising in temporal proximity to ingestion of any
type of food ("generalists")
- Patients who develop anaphylaxis with exercise only with ingestion of a specific food ("specialists")
Foods associated with FDEIA
Wheat is the most common food associated with food-dependent exercise-induced anaphylaxis (FDEIA). Both exercise and aspirin-intake facilitate allergen absorption from the gastrointestinal tract.
80% of the patients with wheat-induced FDEIA have IgE reacting to omega-5 gliadin and the remaining of the patients to high molecular weight glutenin (HMW-glutenin).
Foods associated with FDEIA
- Wheat. Prevalence of wheat allergy in Japan is 0.2% - the assessment was based on questionnaire-based exam, skin prick test, and omega-5 gliadin sIgE (http://goo.gl/Mp4nW).
- Buckwheat
- Crustaceans
- Cephalopods
- Celery
- Chicken
- Grapes
- Tomato
- Dairy products
- Mushrooms
Management of FDEIA
Management of FDEIA
Management of food-dependent EIA includes:
- avoiding exercising in proximity to food consumption (4-6 hours)
- carrying self-injectable epinephrine (EpiPen)
- exercising with a partner
- wearing a medical alert bracelet which lists the condition FDEIA and treatment (EpiPen)
Which of the following foods is often associated with food-dependent exercise-induced anaphylaxis (FDEIA)?
(A) peanut
(B) fish
(C) wheat
(D) soy
(E) egg
(F) milk
Answer: C.
Please note that FDEIA is different from exercise-induced bronchospasm (EIB) (click to enlarge the image):
References
Food-Dependent Exercise-Induced Anaphylaxis-Importance of Omega-5 Gliadin and HMW-Glutenin as Causative Antigens for Wheat-Dependent Exercise-Induced Anaphylaxis. Morita E, Matsuo H, Chinuki Y, Takahashi H, Dahlström J, Tanaka A. Allergol Int. 2009 Oct 25;58(4).
LTP and PG2A are tomato allergens http://goo.gl/C4Hhv
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Key figures: New nomenclature and classification of gluten-related disorders and Algorithm for the differential diagnosis of gluten-related disorders, including celiac disease, gluten sensitivity and wheat allergy. BMC Medicine 2012.
Published: 05/09/2010
Updated: 02/09/2012
Key figures: New nomenclature and classification of gluten-related disorders and Algorithm for the differential diagnosis of gluten-related disorders, including celiac disease, gluten sensitivity and wheat allergy. BMC Medicine 2012.
Published: 05/09/2010
Updated: 02/09/2012
Interleukin 33 (IL-33)
Author: V. Dimov, M.D., Allergist/Immunologist, Assistant Professor, University of Chicago
Reviewer: S. Randhawa, M.D.
Interleukin 33 (IL-33) is a cytokine belonging to the IL-1 superfamily, it induces cells to produce type 2 cytokines.
Interleukin-1 superfamily
Interleukin-1 superfamily includes:
- IL-1α
- IL-1β and IL-1RA
- IL1F5, IL1F6, IL1F7, IL1F8, IL1F9, and IL1F10
- IL-33
- IL-18
IL-1α, IL-1β, and IL-1RA have been renamed IL-1F1, IL-1F2, and IL-1F3. IL-33 is also called IL-1F11.
Whereas IL-1 and IL-18 promote proinflammatory and TH1-associated responses, IL-33 induces the production of TH2-associated cytokines.
IL-33 was previously named NF-HEV nuclear factor (NF) in high endothelial venules (HEVs) since it was originally identified in this location. IL-33 is also called IL-1F11 to note its place as a member of IL-1 superfamily (IL-1F11).
IL-33 binds to its receptors triggering NF-κB and MAP kinase signaling pathways that drive production of type 2 cytokines (IL-5 and IL-13) from Th2 cells.
Receptors for IL-33
IL-33 binds to 2 receptors:
- ST2 (IL1RL1)
- IL-1 Receptor Accessory Protein (IL1RAP)
ST2 (IL1RL1)
IL1RL1 stands for IL-1 receptor-like 1 protein. Mutations in the gene for IL1RL1 (ST2) have been linked to atopic dermatitis and asthma.
ST2 is also called IL1RL1, T1, DER4 and Fit-2. ST2 is highly expressed on mast cells and on TH2 cells.
The ST2 gene encodes two isoforms of ST2 proteins:
- ST2L, a transmembrane form
- soluble ST2 (sST2), a secreted form that can serve as a decoy receptor of IL-33
High levels of sST2 has been found in the sera of patients with acute asthma.
IL-33 is markedly elevated in the serum of patients during an anaphylactic shock and in atopic human tissue.
IL-33 activates:
- Phospholipase D1 (PLD1)
- Sphingosine kinase 1 (SPHK1)
Phospholipase D1 (PLD1)
Phospholipase D1 (PLD1) catalyzes the hydrolysis of phosphatidylcholine (PC) to produce phosphatidic acid and choline. PC-specific PLD1 affects numerous cellular pathways, including signal transduction, membrane trafficking, and the regulation of mitosis.
Sphingosine-1-phosphate (S1P) and Sphingosine kinase 1 (SPHK1)
Sphingosine-1-phosphate (S1P) is a signaling sphingolipid. Various stimuli increase cellular levels of S1P by activation of sphingosine kinase (SPHK), the enzyme that catalyzes the phosphorylation of sphingosine.
S1P regulates angiogenesis, vascular stability and permeability.
S1P is a major regulator of trafficking of T- and B-cells. S1P interaction with its receptor S1PR1 is needed for the egress of immune cells from the lymphoiod organs (such as thymus and lymph nodes). Some immunosuppessants such as FTY720 do not let lymphocytes leave the lymph nodes through blockage of S1PR. Fingolimod works in multiple sclerosis by binding to S1P receptors and acting as highly potent antagonist (NEJM, 2012).
In the presence of IgE, IL-33 activates mast cell degranulation through phospholipase
D1 and sphingosine kinase-1.
IL-33 expression is increased in patients with anaphylaxis and atopic dermatitis.
IL-33 is a potential therapeutic target against allergy. IL-33/ST2 pathway may provide new therapeutic targets for allergic rhinitis and asthma (http://goo.gl/3utyB).
NFkB dependent and independent cytokines and chemokines
It has been suggested that whilst the production of pro-inflammatory cytokines in mast
cells is NFkB dependent, the induction of Th2 cytokines is NFkB independent.
For example, IL-1, IL-3, IL-6, TNF-alpha, MIP-2, MCP-1, and MIP-1 syntheses are dependent on NF-kB activity. IL-5, IL-13, Eotaxin-2, RANTES or TARC syntheses are are independent of the NF-kB pathway.
Abbreviations
Chemokine (C-X-C motif) ligand 2 (CXCL2) is a small cytokine belonging to the CXC chemokine family that is also called macrophage inflammatory protein 2-alpha (MIP2-alpha), Growth-regulated protein beta (Gro-beta) and Gro oncogene-2 (Gro-2).
Chemokine (C-C motif) ligand 2 (CCL2) is a small cytokine belonging to the CC chemokine family that is also known as monocyte chemotactic protein-1 (MCP-1).
Chemokine (C-C motif) ligand 4 is also known as CCL4 and MIP-1.
Chemokine (C-C motif) ligand 24 (CCL24) is a small cytokine belonging to the CC chemokine family that is also known as Myeloid progenitor inhibitory factor 2 (MPIF-2) and Eosinophil chemotactic protein 2 (Eotaxin-2). CCL24 interacts with chemokine receptor CCR3 to induce chemotaxis in eosinophils.
Chemokine (C-C motif) ligand 5 also known as CCL5 or RANTES. CCL5 was earlier called Regulated upon Activation, Normal T-cell Expressed, and Secreted, abbreviated RANTES.
Chemokine (C-C motif) ligand 17 (CCL17) is a small cytokine belonging to the CC chemokine family that is also known as thymus and activation regulated chemokine (TARC).
IL-33 role in anaphylaxis
In the presence of IgE, IL-33 induces anaphylactic shock by rapidly activating mast cell degranulation. Although mast cell activation and degranulation by IL-33 is independent of the presence of T or B cells, the presence of preformed IgE is critical. In vitro the IgE sensitization need to be for at least 16 hours, and shorter sensitization durations failed to primed the mast cells for IL-33–mediated degranulation.
References
The cytokine interleukin-33 mediates anaphylactic shock. Pushparaj PN, Tay HK, H'ng SC, Pitman N, Xu D, McKenzie A, Liew FY, Melendez AJ. Proc Natl Acad Sci U S A. 2009 Jun 16;106(24):9773-8. Epub 2009 Jun 8.
IL-33 and its receptor ST2 play important roles in allergic rhinitis http://goo.gl/xYCga
Published: 08/25/2009
Updated: 01/07/2012
Reviewer: S. Randhawa, M.D.
Interleukin 33 (IL-33) is a cytokine belonging to the IL-1 superfamily, it induces cells to produce type 2 cytokines.
Interleukin-1 superfamily
Interleukin-1 superfamily includes:
- IL-1α
- IL-1β and IL-1RA
- IL1F5, IL1F6, IL1F7, IL1F8, IL1F9, and IL1F10
- IL-33
- IL-18
IL-1α, IL-1β, and IL-1RA have been renamed IL-1F1, IL-1F2, and IL-1F3. IL-33 is also called IL-1F11.
Whereas IL-1 and IL-18 promote proinflammatory and TH1-associated responses, IL-33 induces the production of TH2-associated cytokines.
IL-33 was previously named NF-HEV nuclear factor (NF) in high endothelial venules (HEVs) since it was originally identified in this location. IL-33 is also called IL-1F11 to note its place as a member of IL-1 superfamily (IL-1F11).
IL-33 binds to its receptors triggering NF-κB and MAP kinase signaling pathways that drive production of type 2 cytokines (IL-5 and IL-13) from Th2 cells.
Receptors for IL-33
IL-33 binds to 2 receptors:
- ST2 (IL1RL1)
- IL-1 Receptor Accessory Protein (IL1RAP)
ST2 (IL1RL1)
IL1RL1 stands for IL-1 receptor-like 1 protein. Mutations in the gene for IL1RL1 (ST2) have been linked to atopic dermatitis and asthma.
ST2 is also called IL1RL1, T1, DER4 and Fit-2. ST2 is highly expressed on mast cells and on TH2 cells.
The ST2 gene encodes two isoforms of ST2 proteins:
- ST2L, a transmembrane form
- soluble ST2 (sST2), a secreted form that can serve as a decoy receptor of IL-33
High levels of sST2 has been found in the sera of patients with acute asthma.
IL-33 is markedly elevated in the serum of patients during an anaphylactic shock and in atopic human tissue.
IL-33 activates:
- Phospholipase D1 (PLD1)
- Sphingosine kinase 1 (SPHK1)
Phospholipase D1 (PLD1)
Phospholipase D1 (PLD1) catalyzes the hydrolysis of phosphatidylcholine (PC) to produce phosphatidic acid and choline. PC-specific PLD1 affects numerous cellular pathways, including signal transduction, membrane trafficking, and the regulation of mitosis.
Sphingosine-1-phosphate (S1P) and Sphingosine kinase 1 (SPHK1)
Sphingosine-1-phosphate (S1P) is a signaling sphingolipid. Various stimuli increase cellular levels of S1P by activation of sphingosine kinase (SPHK), the enzyme that catalyzes the phosphorylation of sphingosine.
S1P regulates angiogenesis, vascular stability and permeability.
S1P is a major regulator of trafficking of T- and B-cells. S1P interaction with its receptor S1PR1 is needed for the egress of immune cells from the lymphoiod organs (such as thymus and lymph nodes). Some immunosuppessants such as FTY720 do not let lymphocytes leave the lymph nodes through blockage of S1PR. Fingolimod works in multiple sclerosis by binding to S1P receptors and acting as highly potent antagonist (NEJM, 2012).
In the presence of IgE, IL-33 activates mast cell degranulation through phospholipase
D1 and sphingosine kinase-1.
IL-33 expression is increased in patients with anaphylaxis and atopic dermatitis.
IL-33 is a potential therapeutic target against allergy. IL-33/ST2 pathway may provide new therapeutic targets for allergic rhinitis and asthma (http://goo.gl/3utyB).
NFkB dependent and independent cytokines and chemokines
It has been suggested that whilst the production of pro-inflammatory cytokines in mast
cells is NFkB dependent, the induction of Th2 cytokines is NFkB independent.
For example, IL-1, IL-3, IL-6, TNF-alpha, MIP-2, MCP-1, and MIP-1 syntheses are dependent on NF-kB activity. IL-5, IL-13, Eotaxin-2, RANTES or TARC syntheses are are independent of the NF-kB pathway.
Abbreviations
Chemokine (C-X-C motif) ligand 2 (CXCL2) is a small cytokine belonging to the CXC chemokine family that is also called macrophage inflammatory protein 2-alpha (MIP2-alpha), Growth-regulated protein beta (Gro-beta) and Gro oncogene-2 (Gro-2).
Chemokine (C-C motif) ligand 2 (CCL2) is a small cytokine belonging to the CC chemokine family that is also known as monocyte chemotactic protein-1 (MCP-1).
Chemokine (C-C motif) ligand 4 is also known as CCL4 and MIP-1.
Chemokine (C-C motif) ligand 24 (CCL24) is a small cytokine belonging to the CC chemokine family that is also known as Myeloid progenitor inhibitory factor 2 (MPIF-2) and Eosinophil chemotactic protein 2 (Eotaxin-2). CCL24 interacts with chemokine receptor CCR3 to induce chemotaxis in eosinophils.
Chemokine (C-C motif) ligand 5 also known as CCL5 or RANTES. CCL5 was earlier called Regulated upon Activation, Normal T-cell Expressed, and Secreted, abbreviated RANTES.
Chemokine (C-C motif) ligand 17 (CCL17) is a small cytokine belonging to the CC chemokine family that is also known as thymus and activation regulated chemokine (TARC).
IL-33 role in anaphylaxis
In the presence of IgE, IL-33 induces anaphylactic shock by rapidly activating mast cell degranulation. Although mast cell activation and degranulation by IL-33 is independent of the presence of T or B cells, the presence of preformed IgE is critical. In vitro the IgE sensitization need to be for at least 16 hours, and shorter sensitization durations failed to primed the mast cells for IL-33–mediated degranulation.
What is the most potent chemokine (chemoattractant) for eosinophils?
(A) IL-5
(B) IL-8
(C) LTB4
(D) eotaxin
(E) IL-4
(F) IL-13
Answer: D.
Eosinophil chemotactic protein 2 (Eotaxin-2) is the most potent chemoattractant for eosinophils but IL-5 is the most specific stimulant of their production.
References
The cytokine interleukin-33 mediates anaphylactic shock. Pushparaj PN, Tay HK, H'ng SC, Pitman N, Xu D, McKenzie A, Liew FY, Melendez AJ. Proc Natl Acad Sci U S A. 2009 Jun 16;106(24):9773-8. Epub 2009 Jun 8.
IL-33 and its receptor ST2 play important roles in allergic rhinitis http://goo.gl/xYCga
Published: 08/25/2009
Updated: 01/07/2012
Anaphylaxis
 Editor: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Editor: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of ChicagoInformation For Patients
Anaphylaxis
How to use Auvi-Q or EpiPen (video)
Action plan for anaphylaxis
Allergy Testing
Allergic Reactions
Anaphylaxis Checklist
Are you food allergy aware - Ana & Phil Axis (PDF)
What to expect when visiting an allergy clinic
Current allergy skin tests are virtually painless. This video by Dr. Bassett, a board-certified allergist from New York City, shows what to expect when visiting an allergy clinic for diagnosis and treatment:
Information For Doctors
Anaphylaxis: Teaching Cases
Anaphylactic Shock Due to Bee Sting
Anaphylactic reaction to subcutaneous immunotherapy: what to do?
Anaphylactoid Reaction to Intravenous Contrast
Large Skin Reaction to Insect Bites and Stings: Is it Dangerous and What to Do?
How to Diagnose Latex Allergy
How to manage indolent systemic mastocytosis (ISM)?
Related Reading
Idiopathic anaphylaxis
Anaphylaxis: Brief Review
Mind Maps: Anaphylaxis
Simplified algorithm for the acute management of anaphylaxis. Allergy, Asthma & Clinical Immunology 2011 7(Suppl 1):S6.
Mnemonics: Anaphylaxis
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Anaphylaxis Australia
Anaphylaxis - UK NICE guidelines
Blog articles from AllergyNotes
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
Image source: Bee, Wikipedia, GNU Free Documentation License.
{kind=link}
Published: 07/01/2007
Updated: 05/15/2014
Large Skin Reaction to Insect Bites and Stings: Is it Dangerous and What to Do?
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 55-year-old male followed by the clinic for allergic rhinitis and asthma called the allergist on call with complaints of 5 recent insect bites/stings. He was working on his house (in August) when he was bitten by 5 insects: 4 of them slightly larger than flies and one which looked like a bee. He was bitten 5 hours ago, and now has edema and pain in the following areas: L cheek halfway to the jaw, left thumb, left little finger, right shin, and left hip, about 3 inches in size. He reports no SOB, wheezing, dizziness or fever. He did not see any stings left in the affected areas.
The patient put ice packs on the swellings and wants to know if anything else should be done.


A yellow jacket wasp with a typical narrow waist (left) and a honey bee with a fat hairy "fuzzy" body (right). Image source: Wikipedia 1, 2, GNU Free Documentation License.
Past medical history (PMH)
Allergic rhinitis, skin prick test positive for molds and grass, asthma, hypertension (HTN).
Medications
Nasonex, Advair, Allegra, Amlodipine, triamcinolone lotion.
What is the most likely diagnosis?
Local reactions to insect bites/stings.
What is the strongest predictor of benign outcome of insect bites in this patient?
The long time frame. For example, most fatalities from wasp stings occur within an hour of the sting.
What advice would you give to this patient?
He had already taken an antihistamine (Allegra). He was advised to put triamcinolone lotion on the affected areas and to continue using the ice packs.
He reported large local reactions to bee stings several years ago but had no systemic symptoms at the time. The patient was asked to make an appointment for insect venom testing in 6 weeks.
Final diagnosis
Local reactions to insect bites/stings.
Summary
Skin testing
Skin testing in insect venom anaphylaxis is done 6 weeks after the sting.
Suggested indications for skin test with insect venom allergens:
- history of systemic reaction
- a local reaction away from the place of the sting ("a satellite")
- very large local reaction
- history of multiple stings on several occasions in the past
How to do skin testing in insect venom allergy - prick or intradermal?
Venom testing is performed initially with prick tests. If results are negative, intradermal testing is used with a concentration in the range of 0.001 to 0.01 µg/mL.
Skin test may be negative during the first 6 weeks after a sting due to a refractory period or "anergy."
Skin tests and RAST are complementary, as neither test alone will detect all patients with insect sting allergy.
Local Reactions
Large local reactions occur in 17-56% of stung people. The localized reaction may last 12-24 hours.
How do you define a large local reaction to insect sting?
- increase in size for 24 to 48 hours,
- swelling to more than 10 cm in diameter
- 5 to 10 days to resolve
Patients who have experienced large local reactions often have large local
reactions to subsequent stings, and up to 10% might eventually have a systemic reaction.
What is the difference between a large local reaction and a systemic cutaneous reaction?
Systemic reactions can include a spectrum of manifestations ranging from mild to life-threatening:
- cutaneous reactions (eg, urticaria and angioedema),
- bronchospasm
- large airway obstruction (tongue or throat swelling, laryngeal edema)
- hypotension and shock.
The key feature that distinguishes a systemic cutaneous reaction from a large local reaction is the involvement of parts of the body not contiguous with the site of the sting.
Large local reactions to stings have a 4-10% chance of a future systemic reaction. According to more recent studies, large local reactions (LLRs) from stinging insects are followed by a systemic reaction in 10-15% of patients. Prescription of autoinjectable adrenaline is advisable in large LLRs due to insects, immunotherapy studies needed http://bit.ly/HhmUo
Local reactions may be life threatening if local swelling at the sting site compromises the airway. Edema may extend to 10 cm from site of the sting.
Topical antihistamines should not be used because they may penetrate the wounded skin, bind to proteins and cause sensitization through haptenization.

Mind map of insect venom allergy.
Systemic Reactions
In one study, 1-2% of the people experienced a generalized reaction, and 5% sought medical care. 3% of adults and less than 1% of children have systemic reactions to wasp stings. Adults are at a higher risk because they are more likely to have developed sensitization from a prior wasp sting.
Children generally have a more benign course after insect stings because they usually have only cutaneous systemic reactions. Remember:
C
Children
Cutaneous only
A
Adults
Airway
Anaphylaxis
Wasps and bees cause 30-120 deaths yearly in the United States.
Systemic reactions to stings are rapid: 50% of deaths occur within 30 minutes of the sting, and 75% occur within 4 hours.
In wasp stings, most deaths occur within 1 hour, with most severe reactions occurring within 10 minutes of the wasp sting. The systemic reaction is more related to the pre-existing level of circulating IgE rather than to the number of wasp stings.
Epinephrine, systemic steroids and ER care should be considered early in patients with systemic symptoms.
Acute management of anaphylaxis
Drugs: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing; IV fluids if hypotensive

Mind map diagram of anaphylaxis.
All patients with history of systemic reaction to insect stings should be prescribed EpiPen Twin Pack.
EpiPen delivers epinephrine within seconds to minutes and "buys" the victim 20 minutes to get to the nearest emergency room. EpiPens expire every 18 months and it is recommended to have 2 of them handy.
References
Stinging Insect Hypersensitivity: A Practice parameter Update. Joint Council of Allergy, Asthma, and Immunology.
Insect Bites. Dirk M Elston. eMedicine.
Bee and Hymenoptera Stings. Hemant H Vankawala, Randy Park. eMedicine.
Wasp Stings. Carl A Mealie. eMedicine.
Anaphylactic Shock Due to Bee Sting
Venom Allergy: A Short Review.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Insect sting anaphylaxis. David B.K. Golden. Immunol Allergy Clin North Am. 2007 May; 27(2): 261–vii.
Hymenoptera Venom Allergy. Velma Paschall. Cleveland Clinic.
Insect Stings. NEJM, Volume 331:523-527, August 25, 1994.
Insect Stings and Bites. Ask the Expert. AAAAI.
Insect Sting. Ask the Expert. AAAAI.
Insect Sensitivity. Ask the Expert. AAAAI.
Insect Bite. Ask the Expert. AAAAI.
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 55-year-old male followed by the clinic for allergic rhinitis and asthma called the allergist on call with complaints of 5 recent insect bites/stings. He was working on his house (in August) when he was bitten by 5 insects: 4 of them slightly larger than flies and one which looked like a bee. He was bitten 5 hours ago, and now has edema and pain in the following areas: L cheek halfway to the jaw, left thumb, left little finger, right shin, and left hip, about 3 inches in size. He reports no SOB, wheezing, dizziness or fever. He did not see any stings left in the affected areas.
The patient put ice packs on the swellings and wants to know if anything else should be done.

A yellow jacket wasp with a typical narrow waist (left) and a honey bee with a fat hairy "fuzzy" body (right). Image source: Wikipedia 1, 2, GNU Free Documentation License.
{kind=link}
Past medical history (PMH)
Allergic rhinitis, skin prick test positive for molds and grass, asthma, hypertension (HTN).
Medications
Nasonex, Advair, Allegra, Amlodipine, triamcinolone lotion.
What is the most likely diagnosis?
Local reactions to insect bites/stings.
What is the strongest predictor of benign outcome of insect bites in this patient?
The long time frame. For example, most fatalities from wasp stings occur within an hour of the sting.
What advice would you give to this patient?
He had already taken an antihistamine (Allegra). He was advised to put triamcinolone lotion on the affected areas and to continue using the ice packs.
He reported large local reactions to bee stings several years ago but had no systemic symptoms at the time. The patient was asked to make an appointment for insect venom testing in 6 weeks.
Final diagnosis
Local reactions to insect bites/stings.
Summary
Skin testing
Skin testing in insect venom anaphylaxis is done 6 weeks after the sting.
Suggested indications for skin test with insect venom allergens:
- history of systemic reaction
- a local reaction away from the place of the sting ("a satellite")
- very large local reaction
- history of multiple stings on several occasions in the past
How to do skin testing in insect venom allergy - prick or intradermal?
Venom testing is performed initially with prick tests. If results are negative, intradermal testing is used with a concentration in the range of 0.001 to 0.01 µg/mL.
Skin test may be negative during the first 6 weeks after a sting due to a refractory period or "anergy."
Skin tests and RAST are complementary, as neither test alone will detect all patients with insect sting allergy.
Local Reactions
Large local reactions occur in 17-56% of stung people. The localized reaction may last 12-24 hours.
How do you define a large local reaction to insect sting?
- increase in size for 24 to 48 hours,
- swelling to more than 10 cm in diameter
- 5 to 10 days to resolve
Patients who have experienced large local reactions often have large local
reactions to subsequent stings, and up to 10% might eventually have a systemic reaction.
What is the difference between a large local reaction and a systemic cutaneous reaction?
Systemic reactions can include a spectrum of manifestations ranging from mild to life-threatening:
- cutaneous reactions (eg, urticaria and angioedema),
- bronchospasm
- large airway obstruction (tongue or throat swelling, laryngeal edema)
- hypotension and shock.
The key feature that distinguishes a systemic cutaneous reaction from a large local reaction is the involvement of parts of the body not contiguous with the site of the sting.
Large local reactions to stings have a 4-10% chance of a future systemic reaction. According to more recent studies, large local reactions (LLRs) from stinging insects are followed by a systemic reaction in 10-15% of patients. Prescription of autoinjectable adrenaline is advisable in large LLRs due to insects, immunotherapy studies needed http://bit.ly/HhmUo
Local reactions may be life threatening if local swelling at the sting site compromises the airway. Edema may extend to 10 cm from site of the sting.
Topical antihistamines should not be used because they may penetrate the wounded skin, bind to proteins and cause sensitization through haptenization.

Mind map of insect venom allergy.
Systemic Reactions
In one study, 1-2% of the people experienced a generalized reaction, and 5% sought medical care. 3% of adults and less than 1% of children have systemic reactions to wasp stings. Adults are at a higher risk because they are more likely to have developed sensitization from a prior wasp sting.
Children generally have a more benign course after insect stings because they usually have only cutaneous systemic reactions. Remember:
C
Children
Cutaneous only
A
Adults
Airway
Anaphylaxis
Wasps and bees cause 30-120 deaths yearly in the United States.
Systemic reactions to stings are rapid: 50% of deaths occur within 30 minutes of the sting, and 75% occur within 4 hours.
In wasp stings, most deaths occur within 1 hour, with most severe reactions occurring within 10 minutes of the wasp sting. The systemic reaction is more related to the pre-existing level of circulating IgE rather than to the number of wasp stings.
Epinephrine, systemic steroids and ER care should be considered early in patients with systemic symptoms.
Acute management of anaphylaxis
Drugs: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing; IV fluids if hypotensive

Mind map diagram of anaphylaxis.
All patients with history of systemic reaction to insect stings should be prescribed EpiPen Twin Pack.
EpiPen delivers epinephrine within seconds to minutes and "buys" the victim 20 minutes to get to the nearest emergency room. EpiPens expire every 18 months and it is recommended to have 2 of them handy.
References
Stinging Insect Hypersensitivity: A Practice parameter Update. Joint Council of Allergy, Asthma, and Immunology.
Insect Bites. Dirk M Elston. eMedicine.
Bee and Hymenoptera Stings. Hemant H Vankawala, Randy Park. eMedicine.
Wasp Stings. Carl A Mealie. eMedicine.
Anaphylactic Shock Due to Bee Sting
Venom Allergy: A Short Review.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Insect sting anaphylaxis. David B.K. Golden. Immunol Allergy Clin North Am. 2007 May; 27(2): 261–vii.
Hymenoptera Venom Allergy. Velma Paschall. Cleveland Clinic.
Insect Stings. NEJM, Volume 331:523-527, August 25, 1994.
Insect Stings and Bites. Ask the Expert. AAAAI.
Insect Sting. Ask the Expert. AAAAI.
Insect Sensitivity. Ask the Expert. AAAAI.
Insect Bite. Ask the Expert. AAAAI.
Related reading
Beebearding is thought to date back to the 1700s http://goo.gl/j4nE
Stinging Insect Guidelines - 2001 Update by AAAAI and ACAAI. Medscape, 2011.
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Published: 08/25/2008
Updated: 06/15/2011
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Published: 08/25/2008
Updated: 06/15/2011
Anaphylactic reaction to subcutaneous immunotherapy: what to do?
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 31-year-old Caucasian male has been on subcutaneous immunotherapy for allergic rhinitis for 3 months. The subcutaneous immunotherapy (SCIT) consists of 3 injections with extracts of grasses, trees, weeds (vial A), dust mite, molds (vial B), cat and ragweed (vial C). His maintenance dose goal is 0.5 ml.
The SCIT dose was gradually increased with weekly injections and the dose he received last week was 0.3 ml. The patient reports large local reactions which started at the level of 0.1 ml and increased progressively as the dose increased to 0.2 ml.
During the last visit, the size of the local reaction was 30 x 30 mm in terms of swelling. He has no history of prior systemic reactions to SCIT.
Past medical history (PMH)
Allergic rhinitis. He has a remote history of mild asthma, which has been asymptomatic for years and he used only occasionally a prn albuterol inhaler in the remote past.
Medications
Benadryl PRN, Flonase (fluticasone) nasal spray daily
What happened?
The patient received three injections of immunotherapy today at 10:50 and within two to three minutes of the injection, he started to complain of feeling that his throat was closing, dry cough and itchy eyes. He was evaluated immediately by the nurses and his allergist.
What is the most likely diagnosis?
He was found to have an anaphylactic reaction to the subcutaneous immunotherapy.
What treatment would you suggest?
He was given a dose of epineprine 0.3 mg IM at 10:51 and Alavert 10 mg po dissolvable tablet at 10:52. At that time, his blood pressure was 140/55, heart rate was 112, and his pulse-oximetry was 93% on room air.
At 11:00, he was given 40 mg of prednisone po x 1.
What happened next?
The patient reported that his throat sensation was better; however, his pulse-oximetry was noted to be in the range of 90% and on physical examination, he developed diffuse bilateral expiratory wheezing. The physical examination was also remarkable for conjunctival injection and development of swelling around the injection site on both arms with large, local reaction in the range of 8 to 9 cm on the left arm with wheals and satellite wheals around the injection sites.
What treatment would you suggest next?
He was treated with albuterol four puffs at 11:15. At 11:20, he reported improvement in his throat sensation and shortness of breath. His pulse-oximetry was 96%; blood pressure was 130/80.
At 11:30, the patient reportedly returned to baseline in terms of his symptoms. On physical examination, he had no more wheezing.
He was given a prescription for prednisone 40 mg po daily for three days and loratadine 10 mg po daily for seven days.
How would you change the immunotherapy prescription?
His dose of immunotherapy was returned to the dose two steps before the current one, which was 0.1 ml and he is to stay on this dose for two months.
The patient was discharged from the clinic at 12:50, two hours after the event. He is on prednisone, which should prevent any symptoms of late reaction.
Final diagnosis
Anaphylactic reaction to subcutaneous immunotherapy
Summary
Anaphylaxis mind map diagram.
Allergen immunotherapy was introduced by Leonard Noon 100 years ago and is the only disease-modifying treatment for allergic individuals (Allergy, 2012).
During a retrospective chart review of 388 patients, the rate of systemic reactions during subcutaneous immunotherapy was 0.28% per injection and 7.4% per patient. It was concerning that 48% of the systemic reactions occurred more than 30 minutes after the injection and many of these reactions required epinephrine.
This study was unable to identify risk factors that predict the reactions. Gender, phase (build-up versus maintenance), asthma, angiotensin-converting enzyme inhibitors, beta-blockers, initial skin-prick test size, or allergen type did not increase the odds of a systemic reaction.
Skin prick testing (SPT) on beta-blockers was safe in 199 patients in a 2012 study (http://goo.gl/3vGSl). However, incidence of systemic reactions is 1:250 with SPT.
Mnemonics for anaphylaxis
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References
Allergen immunotherapy safety: Characterizing systemic reactions and identifying risk factors. Rank, Mathew A.; Oslie, Corrine L.; Krogman, Jennifer L.; Park, Miguel A.; Li, James T. Allergy and Asthma Proceedings, Volume 29, Number 4, 7/8 2008 , pp. 400-405(6).
Evaluation of near-fatal reactions to allergen immunotherapy injections. Amin HS, Liss GM, Bernstein DI. J Allergy Clin Immunol. 2006 Jan;117(1):169-75.
Anaphylactic reactions during immunotherapy. Rezvani M, Bernstein DI. Immunol Allergy Clin North Am. 2007 May;27(2):295-307, viii.
Allergen immunotherapy: A practice parameter second update. JACI, 2007 (PDF).
Anaphylaxis: A Short Review
Rate of systemic reactions during subcutaneous immunotherapy: 0.28% per injection
Mnemonics: Anaphylaxis
Mind Maps: Anaphylaxis
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 31-year-old Caucasian male has been on subcutaneous immunotherapy for allergic rhinitis for 3 months. The subcutaneous immunotherapy (SCIT) consists of 3 injections with extracts of grasses, trees, weeds (vial A), dust mite, molds (vial B), cat and ragweed (vial C). His maintenance dose goal is 0.5 ml.
The SCIT dose was gradually increased with weekly injections and the dose he received last week was 0.3 ml. The patient reports large local reactions which started at the level of 0.1 ml and increased progressively as the dose increased to 0.2 ml.
During the last visit, the size of the local reaction was 30 x 30 mm in terms of swelling. He has no history of prior systemic reactions to SCIT.
Past medical history (PMH)
Allergic rhinitis. He has a remote history of mild asthma, which has been asymptomatic for years and he used only occasionally a prn albuterol inhaler in the remote past.
Medications
Benadryl PRN, Flonase (fluticasone) nasal spray daily
What happened?
The patient received three injections of immunotherapy today at 10:50 and within two to three minutes of the injection, he started to complain of feeling that his throat was closing, dry cough and itchy eyes. He was evaluated immediately by the nurses and his allergist.
What is the most likely diagnosis?
He was found to have an anaphylactic reaction to the subcutaneous immunotherapy.
What treatment would you suggest?
He was given a dose of epineprine 0.3 mg IM at 10:51 and Alavert 10 mg po dissolvable tablet at 10:52. At that time, his blood pressure was 140/55, heart rate was 112, and his pulse-oximetry was 93% on room air.
At 11:00, he was given 40 mg of prednisone po x 1.
What happened next?
The patient reported that his throat sensation was better; however, his pulse-oximetry was noted to be in the range of 90% and on physical examination, he developed diffuse bilateral expiratory wheezing. The physical examination was also remarkable for conjunctival injection and development of swelling around the injection site on both arms with large, local reaction in the range of 8 to 9 cm on the left arm with wheals and satellite wheals around the injection sites.
What treatment would you suggest next?
He was treated with albuterol four puffs at 11:15. At 11:20, he reported improvement in his throat sensation and shortness of breath. His pulse-oximetry was 96%; blood pressure was 130/80.
At 11:30, the patient reportedly returned to baseline in terms of his symptoms. On physical examination, he had no more wheezing.
He was given a prescription for prednisone 40 mg po daily for three days and loratadine 10 mg po daily for seven days.
How would you change the immunotherapy prescription?
His dose of immunotherapy was returned to the dose two steps before the current one, which was 0.1 ml and he is to stay on this dose for two months.
The patient was discharged from the clinic at 12:50, two hours after the event. He is on prednisone, which should prevent any symptoms of late reaction.
Final diagnosis
Anaphylactic reaction to subcutaneous immunotherapy
Summary
Anaphylaxis mind map diagram.
Allergen immunotherapy was introduced by Leonard Noon 100 years ago and is the only disease-modifying treatment for allergic individuals (Allergy, 2012).
During a retrospective chart review of 388 patients, the rate of systemic reactions during subcutaneous immunotherapy was 0.28% per injection and 7.4% per patient. It was concerning that 48% of the systemic reactions occurred more than 30 minutes after the injection and many of these reactions required epinephrine.
This study was unable to identify risk factors that predict the reactions. Gender, phase (build-up versus maintenance), asthma, angiotensin-converting enzyme inhibitors, beta-blockers, initial skin-prick test size, or allergen type did not increase the odds of a systemic reaction.
Skin prick testing (SPT) on beta-blockers was safe in 199 patients in a 2012 study (http://goo.gl/3vGSl). However, incidence of systemic reactions is 1:250 with SPT.
Mnemonics for anaphylaxis
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
What are the 4 standardized allergen extracts?
(A) Dog
(B) Trees
(C) Cat
(D) Molds
(E) Dust Mite
(F) Grass
(G) Ragweed
The 4 standardized extracts are Cat, Dust Mite, Grass and Ragweed.
References
Allergen immunotherapy safety: Characterizing systemic reactions and identifying risk factors. Rank, Mathew A.; Oslie, Corrine L.; Krogman, Jennifer L.; Park, Miguel A.; Li, James T. Allergy and Asthma Proceedings, Volume 29, Number 4, 7/8 2008 , pp. 400-405(6).
Evaluation of near-fatal reactions to allergen immunotherapy injections. Amin HS, Liss GM, Bernstein DI. J Allergy Clin Immunol. 2006 Jan;117(1):169-75.
Anaphylactic reactions during immunotherapy. Rezvani M, Bernstein DI. Immunol Allergy Clin North Am. 2007 May;27(2):295-307, viii.
Allergen immunotherapy: A practice parameter second update. JACI, 2007 (PDF).
Anaphylaxis: A Short Review
Rate of systemic reactions during subcutaneous immunotherapy: 0.28% per injection
Mnemonics: Anaphylaxis
Mind Maps: Anaphylaxis
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Published: 02/12/2009
Updated: 06/12/2012
Published: 02/12/2009
Updated: 06/12/2012
Anaphylactic Shock Due to Bee Sting
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 45-year-old African American male (AAM) was taken to the local emergency department (ED) with anaphylactic shock. He was working on his house when he was attacked by bees. He was stung twice and subsequently experienced generalized body hives and decrease in systolic blood pressure (SBP) to the 80s per the emergency medical system (EMS) responders. The patient denied shortness of breath (SOB), nausea or vomiting (N/V), or tongue swelling on admission. There was no prior exposure or allergic reaction. Benadryl 25 mg IV and bolus IV fluids were given by EMS.
Past medical history (PMH)
Alcohol abuse, hypertension (HTN), smoking.
Medications
None.
Physical examination
Drowsy but following commands.
VS: BP 100/50, HR 101, RR 18, SpO2 93% on RA.
HEENT: bilateral swollen upper eyelids, no tongue swelling, posterior oral pharynx visualized.
Chest: CTA (B), no respiratory distress, no crackles or wheezing.
CVS: no murmurs, rubs or gallops, regular rate and rhythm.
Abdomen: Soft, NT, ND, + BS.
Extremities: no c/c/e.
Skin: generalized urticarial rash.
What is the most likely diagnosis?
Anaphylactic shock.
What would you do?
He was given:
Epinephrine 0.3 mg IM
Solumedrol 125mg IV
Benadryl 25 mg IV
What happened next?
The patient started to complain of sore throat. ENT consult was called who attempted to visualize the larynx with a fiberoptic scope but the patient was unable to cooperate due to exaggerated gag reflex.
His voice became hoarse, oxygen saturation decreased and he was re-examined by the ED physician who was not able to visualize the posterior pharynx. The anesthesiology team was called, etomidate and succinylcholine were used for paralysis, and ENT intubated the patient with a rigid laryngoscope on first attempt. Propofol infusion was started. ENT reported significant supraglottic swelling.
MICU team was called and the patient was admitted for mechanical ventilation and further treatment. Post-intubation chest X-ray showed appropriate ET tube placement. CBC and BMP were unremarkable. Urine toxic screen was positive for alcohol, and blood alcohol level was elevated.
The patient was on mechanical ventilation for 2 days and after successful extubation was transferred to a regular medical floor. His hospital course was complicated by delirium tremens due to alcohol withdrawal from which he recovered. He was discharged home with an EpiPen prescription and a follow-up appointment with an allergist.
Final diagnosis
Anaphylactic shock due to allergic reaction to bee sting.
What did we learn from this case?
Drugs used for management of anaphylaxis are remembered by the mnemonic EASI:
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing; IV fluids, if hypotensive
Figure 1. Mind map diagram of anaphylaxis (click to enlarge the image).
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 45-year-old African American male (AAM) was taken to the local emergency department (ED) with anaphylactic shock. He was working on his house when he was attacked by bees. He was stung twice and subsequently experienced generalized body hives and decrease in systolic blood pressure (SBP) to the 80s per the emergency medical system (EMS) responders. The patient denied shortness of breath (SOB), nausea or vomiting (N/V), or tongue swelling on admission. There was no prior exposure or allergic reaction. Benadryl 25 mg IV and bolus IV fluids were given by EMS.
Past medical history (PMH)
Alcohol abuse, hypertension (HTN), smoking.
Medications
None.
Physical examination
Drowsy but following commands.
VS: BP 100/50, HR 101, RR 18, SpO2 93% on RA.
HEENT: bilateral swollen upper eyelids, no tongue swelling, posterior oral pharynx visualized.
Chest: CTA (B), no respiratory distress, no crackles or wheezing.
CVS: no murmurs, rubs or gallops, regular rate and rhythm.
Abdomen: Soft, NT, ND, + BS.
Extremities: no c/c/e.
Skin: generalized urticarial rash.
What is the most likely diagnosis?
Anaphylactic shock.
What would you do?
He was given:
Epinephrine 0.3 mg IM
Solumedrol 125mg IV
Benadryl 25 mg IV
What happened next?
The patient started to complain of sore throat. ENT consult was called who attempted to visualize the larynx with a fiberoptic scope but the patient was unable to cooperate due to exaggerated gag reflex.
His voice became hoarse, oxygen saturation decreased and he was re-examined by the ED physician who was not able to visualize the posterior pharynx. The anesthesiology team was called, etomidate and succinylcholine were used for paralysis, and ENT intubated the patient with a rigid laryngoscope on first attempt. Propofol infusion was started. ENT reported significant supraglottic swelling.
MICU team was called and the patient was admitted for mechanical ventilation and further treatment. Post-intubation chest X-ray showed appropriate ET tube placement. CBC and BMP were unremarkable. Urine toxic screen was positive for alcohol, and blood alcohol level was elevated.
The patient was on mechanical ventilation for 2 days and after successful extubation was transferred to a regular medical floor. His hospital course was complicated by delirium tremens due to alcohol withdrawal from which he recovered. He was discharged home with an EpiPen prescription and a follow-up appointment with an allergist.
Final diagnosis
Anaphylactic shock due to allergic reaction to bee sting.
What did we learn from this case?
Drugs used for management of anaphylaxis are remembered by the mnemonic EASI:
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing; IV fluids, if hypotensive
Figure 1. Mind map diagram of anaphylaxis (click to enlarge the image).
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References
Stinging Insect Hypersensitivity: A Practice parameter Update. Joint Council of Allergy, Asthma, and Immunology.
Venom Allergy: A Short Review. V. Dimov, 08/2007.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Venom Allergy: A Short Review. V. Dimov, 08/2007.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Clinical review: ABC of allergies, Anaphylaxis. Pamela W Ewan. BMJ 1998;316:1442-1445.
Anaphylaxis. eMedicine, 07/2005.
Anaphylaxis to stings and bites. Robert J Heddle. MJA 2006; 185 (5): 290.
Related Reading
CNN: Skateboarder's death underscores insect allergy risks. 5 percent of Americans are at risk for a severe, potentially life-threatening allergic reaction from insect stings http://bit.ly/3PEVtK
Anaphylaxis. eMedicine, 07/2005.
Anaphylaxis to stings and bites. Robert J Heddle. MJA 2006; 185 (5): 290.
Related Reading
CNN: Skateboarder's death underscores insect allergy risks. 5 percent of Americans are at risk for a severe, potentially life-threatening allergic reaction from insect stings http://bit.ly/3PEVtK
Beebearding is thought to date back to the 1700s http://goo.gl/j4nE'
Stinging Insect Matching Game. AAAAI.
Stinging Insect Guidelines - 2001 Update by AAAAI and ACAAI. Medscape, 2011.
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Published: 08/24/2007
Updated: 06/15/2011
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Published: 08/24/2007
Updated: 06/15/2011
Mnemonics: Anaphylaxis
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Common causes of anaphylaxis: FIDL
Foods
Insect stings - bee and wasp
Drugs
Latex rubber
Drugs causing anaphylaxis: AAA CAN
Antibiotics (especially penicillin)
Anesthetic drugs IV
ASA
Contrast media IV
Analgesic opioids
NSAIDs
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension.
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
Published: 01/24/2008
Updated: 05/26/2012
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Common causes of anaphylaxis: FIDL
Foods
Insect stings - bee and wasp
Drugs
Latex rubber
Drugs causing anaphylaxis: AAA CAN
Antibiotics (especially penicillin)
Anesthetic drugs IV
ASA
Contrast media IV
Analgesic opioids
NSAIDs
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension.
Mnemonic for EpiPen dose
30 kg or more
0.3 mg dose of epinephrine (EpiPen)
Epinephrine Auto-Injectors
Dey Pharma is no longer shipping SINGLE EpiPen Auto-Injectors - only 2-PAKs will be available:
2
2-PAK EpiPen
20% of patients need
2nd dose in anaphylaxis
Epinephrine Auto-Injectors
Dey Pharma is no longer shipping SINGLE EpiPen Auto-Injectors - only 2-PAKs will be available:
2
2-PAK EpiPen
20% of patients need
2nd dose in anaphylaxis
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Updated: 05/26/2012
Mind Maps: Anaphylaxis
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Anaphylaxis mind map diagram (click to enlarge the image).
Mind map of venom allergy (click to enlarge the image). References: Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Anaphylaxis mind map diagram (click to enlarge the image).
Mind map of venom allergy (click to enlarge the image). References: Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References and related reading and mind maps
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Simplified algorithm for the acute management of anaphylaxis. Allergy, Asthma & Clinical Immunology 2011 7(Suppl 1):S6.
Published: 01/24/2008
Updated: 06/12/2012
Simplified algorithm for the acute management of anaphylaxis. Allergy, Asthma & Clinical Immunology 2011 7(Suppl 1):S6.
Published: 01/24/2008
Updated: 06/12/2012
Insect Venom Allergy: Brief Review
Author: V. Dimov, M.D., Allergist/Immunologist, Cleveland Clinic
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
There are over 50 reported deaths per year due to insect stings in the U.S. The most common stinging insects are bees and wasps. They can cause severe allergic reactions including anaphylaxis and anaphylactic shock. Reactions to wasp stings are more common than those to bees.
Figure 1. Mind map of insect venom allergy (click to enlarge the image).
Classification
Bee and wasp venoms are different. Both contain hyaluronidase but differ in the content of other allergens. Patients allergic to wasp are rarely allergic to bee.
Sensitization
People are rarely stung by wasps -- once every 10-15 years. Sensitization to wasp venom can occur after a single sting. In contrast, allergy to bee venom occurs after frequent stings by bees. Consequently, most people allergic to bees are beekeepers or neighbors of beekeepers.
IgE antibodies to Hymenoptera venom are present in 20-30% of adults who had an insect sting in the previous 2-3 years.
Table 1. Comparison of allergic reactions to wasp and bee venom.
Figure 2. A yellow jacket wasp with a typical narrow waist (left) and a honey bee with a fat hairy "fuzzy" body (right). Image source: Wikipedia 1, 2, GNU Free Documentation License.
Different Stinging Insects - How to Distinguish Them?
Yellow jackets build their nests in the ground and are encountered during yard work,
farming, and gardening. When you see flying hymenoptera around garbage can or foods, think yellow jacket.
Wasps, yellow jackets and hornets, are scavengers, often at outdoor events where food and drink are being served. When you see flying hymenoptera around garbage can or foods, think yellow jacket.
Honeybees
Domestic honeybees are found in commercial hives. Wild honeybees build their nests in tree hollows or old logs.
Honeybees only sting once -- when they sting, their stinger comes out and they die. Wasps can sting multiple times, they can be aggressive and chase their victims.
Bumblebees are an important cause of sting reactions in some settings. Bumblebee
venom allergy is distinct from honeybee venom allergy and requires specific
testing.
Clinical features
Normal reaction: pain, erythema, a small area of edema (less than to 1 cm diameter).
Allergic reactions can be:
- local
- generalized
Local reactions
Edema can affect a hand/foot or even an entire limb, it can lead to blistering. Symptoms begin within 15 to 30 minutes and arise distant from the site of sting. Not dangerous unless it affects the airway.
How do you define a large local reaction to insect sting?
- increase in size for 24 to 48 hours,
- swelling to more than 10 cm in diameter
- 5 to 10 days to resolve
Patients who have experienced large local reactions often have large local
reactions to subsequent stings, and up to 10% might eventually have a systemic reaction.
What is the difference between a large local reaction and a systemic cutaneous reaction?
Systemic reactions can include a spectrum of manifestations ranging from mild to life-threatening:
- cutaneous reactions (eg, urticaria and angioedema),
- bronchospasm
- large airway obstruction (tongue or throat swelling, laryngeal edema)
- hypotension and shock.
The key feature that distinguishes a systemic cutaneous reaction from a large local reaction is the involvement of parts of the body not contiguous with the site of the sting.
Large local reactions are usually late-phase IgE-mediated, with large severe swelling (8-10 inches in diameter) developing over 24 to 48 hours and resolving in 2-7 days.
Generalized (systemic) reactions
Systemic allergic reactions occur in 1% of children and 3% of adults. Children generally have a more benign course after insect stings because they usually have only cutaneous systemic reactions. Remember:
C
Children
Cutaneous only
A
Adults
Airway
Anaphylaxis
Systemic reactions often start with erythema and pruritus, followed by urticaria and facial or generalized angiooedema.
Patients often feel extremely ill, as if they are going to die ("a sense of impending doom"). SOB can occur due to laryngeal edema or bronchospasm. In severe reactions, hypotension leads to lightheadedness and loss of consciousness. Less common features: abdominal pain, incontinence, chest pain, blurry vision.
The onset of generalized reactions is usually within 10 minutes of a sting.
It is important to check serum tryptase in all patients undergoing workup for venom allergy to rule out indolent mastocytosis.
Only 70% of patients with stinging insect allergy fill their epinephrine prescriptions (Rudders, Annals 2013).
Diagnosis
- History
- Venom-specific IgE antibodies (ImmunoCAP)
Many patients say the sting was from a bee when it is was from an wasp. Vast majority of patients (except beekeepers) will be wasp allergic.
History should be confirmed by demonstrating specific IgE against wasp or bee venom. This is done first by skin test (prick or intradermal) and/or second by blood test (ImmunoCAP).
Skin tests are positive in 65-80% of patients with a history of systemic allergic reactions to insect stings. ImmunoCAP (specific IgE) is less sensitive than venom skin tests and can lead to false positives.
Remember:
Allergy = clinical reactivity
Sensitization = specific IgE antibodies, can occur without clinical reactivity (allergy)
Patients are rarely allergic to both bee and wasp venom.
Extracts
Allergen (venom) vaccine is the recommended term for the therapeutic agent used in allergen immunotherapy. "Vaccine" is used when the therapeutic use of the preparation is
clear. "Extract" is used when the non-therapeutic aspects of the allergen preparation are discussed.
Extracts of honeybee, yellow jacket, white-faced hornet, yellow hornet, and wasp venom are available for skin testing and VIT.
There is no venom extract for fire ant hypersensitivity but a hole-body extract is available.
Tests
Although the negative predictive value of testing in venom allergy is very high, the positive predictive value is much lower.
Baseline serum tryptase is an important predictor of the severity of sting reactions, the frequency of systemic reactions during VIT, the chance of VIT failure, and the risk of relapse if VIT is stopped.
Skin prick tests with a concentration in the range of 1.0 to 100 mcg/mL may be performed before intracutaneous (intradermal) tests but are not used by all allergists.
Intradermal (intracutaneous) tests start with a concentration in the range of 0.001 to 0.01 mcg/mL. If intracutaneous test results at this concentration are negative, the concentration is increased by 10-fold increments until a positive skin test response occurs or a maximum concentration of 1.0 mcg/ mL is reached.
A positive intradermal skin test to insect venom at a concentration of 1.0 mcg/mL or lower is indicative of specific IgE antibodies. False positive results to intradermal testing can occur at venom concentrations greater than 1 mcg/ml, therefore such doses are not recommended for diagnosis.
Skin testing with fire ant whole-body extract is indicative of specific IgE antibodies if a positive response occurs at a concentration of 1:100 wt/vol or less by prick method, or 1:1000 wt/vol or less by intradermal method.
If the skin test is negative despite a convincing history of anaphylaxis after
an insect sting, in vitro testing for IgE antibodies or repeat skin testing is recommended.
Refractory period of “anergy”
Negative skin testing in the days or weeks after a sting reaction may be
Acute management
Drugs: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing
Treatment of choice is epinephrine with a 1:1,000 (1 mg per mL) aqueous solution. Adult dose is 0.3 mL, children dose is 0.01 mg per kg (maximum: 0.3 mL, i.e. one adult dose). Dose can be repeated every 10-15 minutes, up to 2-3 times but in practice repeat administration is generally avoided since high doses of epinephrine can induce arrhythmias.
Patients taking beta blockers can be relatively resistant to epinephrine effect.
Further management
- Desensitization (immunotherapy)
- Self medication with EpiPen
Desensitization (immunotherapy)
Immunotherapy causes a switch from the abnormal Th2 cytokine response to a Th1 response.
Venom immunotherapy has a 98% efficacy but carries a 10% risk systemic allergic reaction and can cause anaphylaxis.
Initial course of weekly injections over 3 months (12 weeks), reaching the highest dose of 100 mcg (equivalent to two stings). Then, maintenance injections of 100 mcg monthly for 5 years. Patients are observed for 30-60 minutes after each injection.
The maintenance dose is 100 mcg for each venom to which the patient has a positive skin test. Mixed vespid venoms (total dose of 300 mcg) are most commonly used.
It is easier to remember that patients come to the office once a week for 12 weeks for their injections. At the end of the 12 weeks, they have been desensitized to the bee stings. Then, they come once a month, for a minimum of five years. Some high-risk patients should be treated indefinitely.
The incidence of systemic reactions with insect venom immunotherapy (10-15%) is similar to inhalant allergen immunotherapy. Less than 50% of reactions require epinephrine injection.
Up to 50% of patients experience large local reactions. Such local reactions are not associated with an increased risk of systemic reactions to subsequent injections.
Venom immunotherapy (VIT)
30-60% of patients with a history of anaphylaxis from an insect sting who have venom-specific IgE antibodies (skin or in vitro testing) will experience a systemic reaction when stung again.
VIT is not necessary in children 16 years of age and younger who have experienced isolated
cutaneous systemic reactions without other systemic manifestations. They only have a 10% chance of having a systemic reaction if stung again, and if one occurs, it is unlikely to be worse
than the initial isolated cutaneous reaction.
VIT in adults who have experienced only cutaneous systemic reaction is controversial but usually recommended.
VIT is extremely effective in reducing the risk of systemic reaction to less than 5%, and sting reactions that occur during VIT are usually milder.
VIT is generally not necessary for patients who have had only a large local reaction because the risk of a systemic reaction is low.
The vast majority of patients who have had a large local reaction do not need to be tested for specific IgE.
What is the dose of VIT?
VIT injections start weekly, beginning with doses no greater than 0.1 to 1.0 mcg, and increasing to a maintenance dose of 100 mcg of each venom (e.g., 1 mL of a vaccine containing 100 mcg/mL of venom).
The dosage schedule for fire ant immunotherapy is less well defined. A maintenance dose
is 0.5 mL of a 1:100 wt/vol concentration.
The interval between maintenance dose injections can be increased to 4-week intervals during the first year of VIT and to every 6 to 8 weeks during subsequent years.
How long to continue VIT?
VIT should be continued for at least 3 to 5 years. Despite the persistence of a positive skin test response, 80-90% of patients will not have a systemic reaction to an insect sting if VIT is stopped after 3 to 5 years.
Some patients with a history of severe anaphylaxis with shock or loss of consciousness still might be at continued risk for a systemic reaction if VIT is stopped, even after
5 years of immunotherapy.
Patients who have experienced a systemic reaction carry injectable epinephrine (eg, EpiPenTM or TwinJectTM devices) at all times.
Patients who take beta-blocker are at greater risk for anaphylaxis to VIT or a sting. Patients who have stinging insect hypersensitivity should not be prescribed beta-blockers unless absolutely necessary.
Self medication
- Oral antihistamines to take as soon as patient is stung
- Syringes preloaded with epinephrine (EpiPen TM)
Epinephrine auto-injector comes in 2 forms: EpiPen, 0.3 mg and EpiPen Jr., 0.15 mg.
EpiPen delivers epinephrine within seconds to minutes and "buys" the victim 20 minutes to get to the nearest emergency room. Some patients will have delayed reactions to the insect venom and this is the reason why they still have to go to the ER to be observed for 3-6 hours.
EpiPens expire every 18 months and it is recommended to have 2 of them handy.
Patient Recommendations
Patients who have a history of a systemic reaction to an insect sting should:
- avoid stinging insects
- carry epinephrine for emergency self-administration
- undergo testing for specific IgE antibodies to stinging insects
- be considered for venom immunotherapy (VIT) if test results for specific IgE antibodies are positive
- carry medical identification of stinging insect hypersensitivity
References
Stinging Insect Hypersensitivity: A Practice parameter Update. Joint Council of Allergy, Asthma, and Immunology.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Stinging Insect Allergy. David B. K. Golden. American Family Physician, June 15, 2003.
Patient information. Tips to Remember: Stinging insect allergy. AAAAI.org.
Anaphylaxis to stings and bites. Robert J Heddle. MJA 2006; 185 (5): 290.
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
There are over 50 reported deaths per year due to insect stings in the U.S. The most common stinging insects are bees and wasps. They can cause severe allergic reactions including anaphylaxis and anaphylactic shock. Reactions to wasp stings are more common than those to bees.
Figure 1. Mind map of insect venom allergy (click to enlarge the image).
Classification
Bee and wasp venoms are different. Both contain hyaluronidase but differ in the content of other allergens. Patients allergic to wasp are rarely allergic to bee.
Sensitization
People are rarely stung by wasps -- once every 10-15 years. Sensitization to wasp venom can occur after a single sting. In contrast, allergy to bee venom occurs after frequent stings by bees. Consequently, most people allergic to bees are beekeepers or neighbors of beekeepers.
IgE antibodies to Hymenoptera venom are present in 20-30% of adults who had an insect sting in the previous 2-3 years.
| Reaction to Wasp | Reaction to Bee |
| More common | Rarer |
| After a single sting | After many stings |
| Typical narrow waist and little hair | Hairy "fuzzy" bee |
Figure 2. A yellow jacket wasp with a typical narrow waist (left) and a honey bee with a fat hairy "fuzzy" body (right). Image source: Wikipedia 1, 2, GNU Free Documentation License.
Different Stinging Insects - How to Distinguish Them?
Yellow jacket, Vespula spp.
Yellow jackets are picnic and trash can scavengers. They are very aggressive, especially
in summer and autumn when larger populations compete for food supplies. They often sting for no apparent reason. Yellow jackets are responsible for most human stings.
Yellow jackets build their nests in the ground and are encountered during yard work,
farming, and gardening. When you see flying hymenoptera around garbage can or foods, think yellow jacket.
Hornets, Dolichovespula arenaria and maculata (yellow hornet and white faced hornets)
Hornets are extremely aggressive and build large nests in trees or shrubs. Nests are often found around human dwellings. Sensitivity to vibrations (e.g. lawn mower) sets off their defensive sting behavior.
Wasp, subfamily Polistinae (paper wasp)
Wasps build honeycomb nests in shrubs and under eaves of houses or barns. Nests are often found on window sills of homes. Wasps have a narrow “wasp waist” and dangling legs when in flight. They are less aggressive but can sting repeatedly without losing sting apparatus.
Honeybees
Domestic honeybees are found in commercial hives. Wild honeybees build their nests in tree hollows or old logs.
Honeybees only sting once -- when they sting, their stinger comes out and they die. Wasps can sting multiple times, they can be aggressive and chase their victims.
Bumblebees are an important cause of sting reactions in some settings. Bumblebee
venom allergy is distinct from honeybee venom allergy and requires specific
testing.
Fire ant, Solenopsis invicta
Fire ants (red or black) are very aggressive and build large nests in mounds of fresh soil which are subterranean. Fire ants widespread in the southeast U.S. They have a true sting apparatus and can deliver multiple stings. Characteristic sterile pustule develop at the site within 24 hours after the sting.
Clinical features
Normal reaction: pain, erythema, a small area of edema (less than to 1 cm diameter).
Allergic reactions can be:
- local
- generalized
Local reactions
Edema can affect a hand/foot or even an entire limb, it can lead to blistering. Symptoms begin within 15 to 30 minutes and arise distant from the site of sting. Not dangerous unless it affects the airway.
How do you define a large local reaction to insect sting?
- increase in size for 24 to 48 hours,
- swelling to more than 10 cm in diameter
- 5 to 10 days to resolve
Patients who have experienced large local reactions often have large local
reactions to subsequent stings, and up to 10% might eventually have a systemic reaction.
What is the difference between a large local reaction and a systemic cutaneous reaction?
Systemic reactions can include a spectrum of manifestations ranging from mild to life-threatening:
- cutaneous reactions (eg, urticaria and angioedema),
- bronchospasm
- large airway obstruction (tongue or throat swelling, laryngeal edema)
- hypotension and shock.
The key feature that distinguishes a systemic cutaneous reaction from a large local reaction is the involvement of parts of the body not contiguous with the site of the sting.
Large local reactions are usually late-phase IgE-mediated, with large severe swelling (8-10 inches in diameter) developing over 24 to 48 hours and resolving in 2-7 days.
Generalized (systemic) reactions
Systemic allergic reactions occur in 1% of children and 3% of adults. Children generally have a more benign course after insect stings because they usually have only cutaneous systemic reactions. Remember:
C
Children
Cutaneous only
A
Adults
Airway
Anaphylaxis
Systemic reactions often start with erythema and pruritus, followed by urticaria and facial or generalized angiooedema.
Patients often feel extremely ill, as if they are going to die ("a sense of impending doom"). SOB can occur due to laryngeal edema or bronchospasm. In severe reactions, hypotension leads to lightheadedness and loss of consciousness. Less common features: abdominal pain, incontinence, chest pain, blurry vision.
The onset of generalized reactions is usually within 10 minutes of a sting.
It is important to check serum tryptase in all patients undergoing workup for venom allergy to rule out indolent mastocytosis.
Only 70% of patients with stinging insect allergy fill their epinephrine prescriptions (Rudders, Annals 2013).
Diagnosis
- History
- Venom-specific IgE antibodies (ImmunoCAP)
Many patients say the sting was from a bee when it is was from an wasp. Vast majority of patients (except beekeepers) will be wasp allergic.
History should be confirmed by demonstrating specific IgE against wasp or bee venom. This is done first by skin test (prick or intradermal) and/or second by blood test (ImmunoCAP).
Skin tests are positive in 65-80% of patients with a history of systemic allergic reactions to insect stings. ImmunoCAP (specific IgE) is less sensitive than venom skin tests and can lead to false positives.
Remember:
Allergy = clinical reactivity
Sensitization = specific IgE antibodies, can occur without clinical reactivity (allergy)
Patients are rarely allergic to both bee and wasp venom.
Extracts
Allergen (venom) vaccine is the recommended term for the therapeutic agent used in allergen immunotherapy. "Vaccine" is used when the therapeutic use of the preparation is
clear. "Extract" is used when the non-therapeutic aspects of the allergen preparation are discussed.
Extracts of honeybee, yellow jacket, white-faced hornet, yellow hornet, and wasp venom are available for skin testing and VIT.
There is no venom extract for fire ant hypersensitivity but a hole-body extract is available.
Tests
Although the negative predictive value of testing in venom allergy is very high, the positive predictive value is much lower.
Baseline serum tryptase is an important predictor of the severity of sting reactions, the frequency of systemic reactions during VIT, the chance of VIT failure, and the risk of relapse if VIT is stopped.
Skin prick tests with a concentration in the range of 1.0 to 100 mcg/mL may be performed before intracutaneous (intradermal) tests but are not used by all allergists.
Intradermal (intracutaneous) tests start with a concentration in the range of 0.001 to 0.01 mcg/mL. If intracutaneous test results at this concentration are negative, the concentration is increased by 10-fold increments until a positive skin test response occurs or a maximum concentration of 1.0 mcg/ mL is reached.
A positive intradermal skin test to insect venom at a concentration of 1.0 mcg/mL or lower is indicative of specific IgE antibodies. False positive results to intradermal testing can occur at venom concentrations greater than 1 mcg/ml, therefore such doses are not recommended for diagnosis.
Skin testing with fire ant whole-body extract is indicative of specific IgE antibodies if a positive response occurs at a concentration of 1:100 wt/vol or less by prick method, or 1:1000 wt/vol or less by intradermal method.
If the skin test is negative despite a convincing history of anaphylaxis after
an insect sting, in vitro testing for IgE antibodies or repeat skin testing is recommended.
Refractory period of “anergy”
Negative skin testing in the days or weeks after a sting reaction may be
due to a refractory period of “anergy”. For these patients, the skin test should be
repeated after 4-6 weeks.
There is no "ideal" test. ImmunoCAP does not correlate perfectly with skin test results, but both tests are useful they supplement each other. Serological testing is negative in up to 20% of skin-positive patients, and skin test are negative in up to 10% of patients found to have venom-specific IgE (positive ImmunoCAP).
There is no "ideal" test. ImmunoCAP does not correlate perfectly with skin test results, but both tests are useful they supplement each other. Serological testing is negative in up to 20% of skin-positive patients, and skin test are negative in up to 10% of patients found to have venom-specific IgE (positive ImmunoCAP).
Patients with a "good" history of venom allergy but negative skin tests should be evaluated with serologic testing. If serological testing is negative, the skin test should be repeated.
Acute management
Drugs: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing
Treatment of choice is epinephrine with a 1:1,000 (1 mg per mL) aqueous solution. Adult dose is 0.3 mL, children dose is 0.01 mg per kg (maximum: 0.3 mL, i.e. one adult dose). Dose can be repeated every 10-15 minutes, up to 2-3 times but in practice repeat administration is generally avoided since high doses of epinephrine can induce arrhythmias.
Patients taking beta blockers can be relatively resistant to epinephrine effect.
Further management
- Desensitization (immunotherapy)
- Self medication with EpiPen
Desensitization (immunotherapy)
Immunotherapy causes a switch from the abnormal Th2 cytokine response to a Th1 response.
Venom immunotherapy has a 98% efficacy but carries a 10% risk systemic allergic reaction and can cause anaphylaxis.
Initial course of weekly injections over 3 months (12 weeks), reaching the highest dose of 100 mcg (equivalent to two stings). Then, maintenance injections of 100 mcg monthly for 5 years. Patients are observed for 30-60 minutes after each injection.
The maintenance dose is 100 mcg for each venom to which the patient has a positive skin test. Mixed vespid venoms (total dose of 300 mcg) are most commonly used.
It is easier to remember that patients come to the office once a week for 12 weeks for their injections. At the end of the 12 weeks, they have been desensitized to the bee stings. Then, they come once a month, for a minimum of five years. Some high-risk patients should be treated indefinitely.
The incidence of systemic reactions with insect venom immunotherapy (10-15%) is similar to inhalant allergen immunotherapy. Less than 50% of reactions require epinephrine injection.
Up to 50% of patients experience large local reactions. Such local reactions are not associated with an increased risk of systemic reactions to subsequent injections.
Venom immunotherapy (VIT)
30-60% of patients with a history of anaphylaxis from an insect sting who have venom-specific IgE antibodies (skin or in vitro testing) will experience a systemic reaction when stung again.
VIT is not necessary in children 16 years of age and younger who have experienced isolated
cutaneous systemic reactions without other systemic manifestations. They only have a 10% chance of having a systemic reaction if stung again, and if one occurs, it is unlikely to be worse
than the initial isolated cutaneous reaction.
VIT in adults who have experienced only cutaneous systemic reaction is controversial but usually recommended.
VIT is extremely effective in reducing the risk of systemic reaction to less than 5%, and sting reactions that occur during VIT are usually milder.
VIT is generally not necessary for patients who have had only a large local reaction because the risk of a systemic reaction is low.
The vast majority of patients who have had a large local reaction do not need to be tested for specific IgE.
What is the dose of VIT?
VIT injections start weekly, beginning with doses no greater than 0.1 to 1.0 mcg, and increasing to a maintenance dose of 100 mcg of each venom (e.g., 1 mL of a vaccine containing 100 mcg/mL of venom).
The dosage schedule for fire ant immunotherapy is less well defined. A maintenance dose
is 0.5 mL of a 1:100 wt/vol concentration.
The interval between maintenance dose injections can be increased to 4-week intervals during the first year of VIT and to every 6 to 8 weeks during subsequent years.
How long to continue VIT?
VIT should be continued for at least 3 to 5 years. Despite the persistence of a positive skin test response, 80-90% of patients will not have a systemic reaction to an insect sting if VIT is stopped after 3 to 5 years.
Some patients with a history of severe anaphylaxis with shock or loss of consciousness still might be at continued risk for a systemic reaction if VIT is stopped, even after
5 years of immunotherapy.
Patients who have experienced a systemic reaction carry injectable epinephrine (eg, EpiPenTM or TwinJectTM devices) at all times.
Patients who take beta-blocker are at greater risk for anaphylaxis to VIT or a sting. Patients who have stinging insect hypersensitivity should not be prescribed beta-blockers unless absolutely necessary.
Self medication
- Oral antihistamines to take as soon as patient is stung
- Syringes preloaded with epinephrine (EpiPen TM)
Epinephrine auto-injector comes in 2 forms: EpiPen, 0.3 mg and EpiPen Jr., 0.15 mg.
EpiPen delivers epinephrine within seconds to minutes and "buys" the victim 20 minutes to get to the nearest emergency room. Some patients will have delayed reactions to the insect venom and this is the reason why they still have to go to the ER to be observed for 3-6 hours.
EpiPens expire every 18 months and it is recommended to have 2 of them handy.
Patient Recommendations
Patients who have a history of a systemic reaction to an insect sting should:
- avoid stinging insects
- carry epinephrine for emergency self-administration
- undergo testing for specific IgE antibodies to stinging insects
- be considered for venom immunotherapy (VIT) if test results for specific IgE antibodies are positive
- carry medical identification of stinging insect hypersensitivity
References
Stinging Insect Hypersensitivity: A Practice parameter Update. Joint Council of Allergy, Asthma, and Immunology.
Clinical review: ABC of allergies, Venom allergy. Pamela W Ewan. BMJ 1998;316:1365-1368.
Stinging Insect Allergy. David B. K. Golden. American Family Physician, June 15, 2003.
Patient information. Tips to Remember: Stinging insect allergy. AAAAI.org.
Anaphylaxis to stings and bites. Robert J Heddle. MJA 2006; 185 (5): 290.
Stinging Insect Guidelines - 2001 Update by AAAAI and ACAAI. Medscape, 2011.
Related reading
'Tongue Drops' Cut Bee Sting Allergy. WebMD, 03/2008.
Fire Ant Stings. Consultant, Vol. 46, No. 13, November 2006.
CNN: Skateboarder's death underscores insect allergy risks. 5 percent of Americans are at risk for a severe, potentially life-threatening allergic reaction from insect stings http://bit.ly/3PEVtK
Related reading
'Tongue Drops' Cut Bee Sting Allergy. WebMD, 03/2008.
Fire Ant Stings. Consultant, Vol. 46, No. 13, November 2006.
CNN: Skateboarder's death underscores insect allergy risks. 5 percent of Americans are at risk for a severe, potentially life-threatening allergic reaction from insect stings http://bit.ly/3PEVtK
Beebearding is thought to date back to the 1700s http://goo.gl/j4nE
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Hymenoptera-Sting Hypersensitivity - NEJM review, 2014 http://buff.ly/1mEZX8z
Videos
Bee Sting Allergies Explained by Robert M. Overholt, M.D. Published: 08/24/2007 Updated: 08/15/2010
Bee Aware Allergy - Insect allergy educational website by Hollister-Stier Laboratories.
Hymenoptera-Sting Hypersensitivity - NEJM review, 2014 http://buff.ly/1mEZX8z
Videos
Bee Sting Allergies Explained by Robert M. Overholt, M.D. Published: 08/24/2007 Updated: 08/15/2010
Anaphylaxis: Brief Review
Author: V. Dimov, M.D., Allergist/Immunologist, Cleveland Clinic
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Figure 1. Mind map diagram of anaphylaxis (click to enlarge the image).
Definition of anaphylaxis
Anaphylaxis was originally described by Portier and Richet in 1902 when the second vaccinating dose of sea anemone toxin caused a dog's death. The response was the opposite of prophylaxis and thus was referred to as anaphylaxis, i.e. "without protection". Anaphylaxis is a severe systemic allergic reaction but there is no universally accepted definition. A good working definition is that anaphylaxis affects more than one organ system, most commonly, skin, respiratory, cardiovascular, and GI systems.
Impact of anaphylaxis
There are 100,000 episodes of anaphylaxis in the U.S. per year, of which almost 1% are fatal (0.65-2%). On average, severe anaphylaxis affects at least 1-3 persons per 10,000 population, and 1-15% of the U.S. population are at risk. An eidemiologic analysis evaluated 464 patients who were hospitalized in Florida for anaphylaxis in 2001. Hospital mortality rate was 0.86%. Median length of stay was 1 day. Median total charges were about $ 5,000. Asthmatics had an increased risk of receiving intubation and mechanical ventilation.
Anaphylaxis is common (1 in 20 adults), 50% never received epineprine, the majority have life-threatening reactions. Anaphylaxis represents a huge opportunity for clinical improvement (Wood, JACI, 2014).
The most common causes of death in anaphylaxis are shock and laryngeal edema. Asthma is a risk factor for fatal outcomes.
Mechanism of anaphylaxis
Anaphylaxis is a type I reaction in the Gell and Goombs classification of hypersensitivity remembered by the mnemonic ACID:
Anaphylaxis, angioedema, asthma, type I
Cytotoxic, antibody-mediated, type II, e.g AIHA, ITP, Graves' disease
Immune complex disease (CIC), type III, e.g. GN, serum sickness
Delayed, cell-mediated, type IV, e.g. contact dermatitis
An allergen reacts with specific IgE antibodies, bound to Fc receptors on mast cells and basophils. This leads to activation of the mast cells and release of mediators responsible for the clinical features of anaphylaxis (BMJ figure).
Rapid release of mediators in anaphylaxis causes the following events remembered by the mnemonic LESS:
Leakage (capilary) --> Urticaria, Angioedema, Laryngeal edema, Hypotension
Edema (mucosal) --> Laryngeal edema, Rhinitis, Wheezing
Smooth muscle contraction --> Wheezing, Abdominal pain
Shock
Increased vascular permeability (capilary leakage) can cause a shift of 50% of vascular volume to the extravascular space within 10 minutes, therefore leading to hypotension and shock. Epinephrine should be administered as early as possible to prevent this fluid shift and shock.
Etiology of anaphylaxis
Foods and insect venom are the 2 most common causes of anaphylaxis. Allergen immunotherapy (desensitization) may also induce anaphylaxis. A total of 46 deaths due to immunotherapy and skin testing were reported from 1945-1987.
Food ingestion is the cause of anaphylaxis in 36% of cases; a medication, allergy immunotherapy, or a diagnostic agent is the cause in 17% of cases; and insect stings are the cause in 15% of cases, 32% are idiopathic.
The common causes of anaphylaxis are remembered by the mneminic FIDL:
Foods - tree nuts, shellfish, 36%
Insect stings - Hymenoptera (bee and wasp), 15%
Drugs - beta-lactams, NSAIDs, 17%
Latex rubber
Anaphylaxis to penicillin (PCN) occurs in 1-5 cases per 10,000 patient treatment courses, with fatalities in 1 case per 50,000-100,000 courses. Insect stings cause 25-50 deaths per year in the U.S.
The largest study of childhood anaphylaxis (as of 2008) included 117 children. Home was the most common setting (48%) and food (85%) the most common trigger. The median age of presentation was 2.4 years. Peanut (18%) and cashew nut (13%) were the most common cause of anaphylaxis.
The 8 top allergens which account for 90 % of all food allergies are remembered by the mnemonic TEMPS WFS:
Tree nuts (almonds, cashews, walnuts)
Egg white (not egg yolk)
Milk
Peanuts
Shellfish (crab, lobster, shrimp)
Wheat
Fish (bass, cod, flounder)
Soy
The most common drugs causing anaphylaxis can be remembered by the mnemonic AAA CAN
Antibiotics (especially penicillin)
Anesthetic drugs, IV
ASA (aspirin)
Contrast media for radiologic studies, IV
Analgesic opioids
NSAIDs
Risk factors for anaphylaxis due to immunotherapy can be remembered by the mnemonic OH BEA:
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Clinical Features of anaphylaxis
The clinical features of anaphylaxis can be remembered by the mnemonic S ECG:
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 25%
Skin: Eythema, Pruritus, Urticaria, Angioedema.
Respiratory: Laryngeal edema, Wheezing, Rhinitis, Conjunctivitis, Itching of palate or external auditory meatus.
Cardiovascular: Palpitations, Sense of impending doom, Fainting, lightheadedness, Collapse, Loss of consciousness.
GI and oral: N/V/D, abdominal pain.
Specific features will often depend on route of allergen entry, for example, insect stings, intravenous drugs can cause cardiovascular problems, especially hypotension and shock. Foods which are absorbed transmucosally can cause lip, facial, and laryngeal edema.
Typically, symptom onset occurs within minutes after exposure and progression is rapid.
Latex rubber anaphylaxis is somewhat unusual because it develops more slowly (30 minutes) as the allergen has to be absorbed through the skin or mucosa.
Diagnosis of anaphylaxis
Anaphylaxis is a clinical diagnosis based on the history of acute exposure to an allergen followed by the typical systemic manifestations. Laboratory studies are not usually required.
Laboratory tests
Platelet-Activating Factor (PAF) may become the "BNP" of anaphylaxis in the future -- a laboratory test which helps in diagnosis. The analogy between PAF and BNP also comes from the fact that both tests help stratify the severity of the disease. The higher then BNP, the more severe the CHF exacerbation is. The same rule applies to PAF.
According to a study published in the NEJM, serum PAF levels were directly correlated with the severity of anaphylaxis. The proportion of subjects with elevated PAF levels increased from 4% in the control groups to 20% in the group with grade 1 anaphylaxis, 71% in the group with grade 2 anaphylaxis, and 100% in the group with grade 3 anaphylaxis.
Management of anaphylaxis
A recent study in the Annals of Allergy, Asthma and Immunology reported on development reported on development of the acronym SAFE, a mnemonic to remind physicians of the 4 action steps for anaphylaxis treatment:
Seek support
Allergen identification and avoidance
Follow-up for specialty care
Epinephrine for emergencies
Drugs used for management of anaphylaxis are remembered by the mnemonic EASI:
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension.
First-line therapy for anaphylaxis is epineprhrine (adrenaline) administered I.M. and it should be given as soon as the condition is recognized. Supplementary therapies include IVF, nebulized bronchodilators, antihistamines and corticosteroids (mnemonic EASI).
Epinephrine should not be given IV except under special circumstances such as profound shock or during anaesthesia. Myocardial infarction has rarely been reported in association with the use of epinephrine. Beta-blockers may increase the severity of an anaphylactic reaction and may antagonize the effect of epinephrine. Use of beta-blockers is not a contraindication to administering epinephrine. Glucagon IM can be administered in patients who take beta-blockers and have developed anaphylaxis.
Bi-phasic anaphylactic reactions have been described but are rare. Administration of steroids should minimize the risk of late relapse. The new guidelines require the prescription of 2 doses of self-injectable epinephrine to all patients (EpiPen 2-Pak).
- Possibly appropriate, subsequent measures depending on response to adrenaline:
- Place patient in recumbent position and elevate lower extremities
- Establish and maintain airway
- Administer oxygen
- Establish venous access
- Normal saline intravenously for fluid replacement
Specific measures to consider after epinephrine injections, where appropriate:
Prevention of anaphylaxis
1. Avoid exposure.
2. Refer to an allergist. Allergy assessment is mandatory in all patients with a history of anaphylaxis to identify and avoid the allergen to prevent its recurrence.
3. Preloaded EpiPen syringes for self treatment of anaphylaxis. Self-injectable epinephrine (adrenaline) should be prescribed in most patients with a history of anaphylaxis. According to a study published in JACI, there were 1,5 million EpiPen prescriptions filled in 2004 with an average of 5.7 EpiPens prescribed per 1000 persons. Massachusetts had the highest number of prescriptions per 1000 persons (11.8), Hawaii had the lowest (2.7). Overall, New England states clearly lead the group with 8-12 EpiPens prescribed per 1000 persons, whereas the southern states had only 3. Authors suggest that the relative lack of sun exposure and vitamin D status may lead to higher incidence of anaphylaxis in the northern states which could explain this strong north-south "gradient."
Patients may be advised to wear a Medic-Alert bracelet with a warning regarding anaphylaxis towards a specific allergen.
References
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Figure 1. Mind map diagram of anaphylaxis (click to enlarge the image).
Definition of anaphylaxis
Anaphylaxis was originally described by Portier and Richet in 1902 when the second vaccinating dose of sea anemone toxin caused a dog's death. The response was the opposite of prophylaxis and thus was referred to as anaphylaxis, i.e. "without protection". Anaphylaxis is a severe systemic allergic reaction but there is no universally accepted definition. A good working definition is that anaphylaxis affects more than one organ system, most commonly, skin, respiratory, cardiovascular, and GI systems.
Impact of anaphylaxis
There are 100,000 episodes of anaphylaxis in the U.S. per year, of which almost 1% are fatal (0.65-2%). On average, severe anaphylaxis affects at least 1-3 persons per 10,000 population, and 1-15% of the U.S. population are at risk. An eidemiologic analysis evaluated 464 patients who were hospitalized in Florida for anaphylaxis in 2001. Hospital mortality rate was 0.86%. Median length of stay was 1 day. Median total charges were about $ 5,000. Asthmatics had an increased risk of receiving intubation and mechanical ventilation.
Anaphylaxis is common (1 in 20 adults), 50% never received epineprine, the majority have life-threatening reactions. Anaphylaxis represents a huge opportunity for clinical improvement (Wood, JACI, 2014).
The most common causes of death in anaphylaxis are shock and laryngeal edema. Asthma is a risk factor for fatal outcomes.
Mechanism of anaphylaxis
Anaphylaxis is a type I reaction in the Gell and Goombs classification of hypersensitivity remembered by the mnemonic ACID:
Anaphylaxis, angioedema, asthma, type I
Cytotoxic, antibody-mediated, type II, e.g AIHA, ITP, Graves' disease
Immune complex disease (CIC), type III, e.g. GN, serum sickness
Delayed, cell-mediated, type IV, e.g. contact dermatitis
An allergen reacts with specific IgE antibodies, bound to Fc receptors on mast cells and basophils. This leads to activation of the mast cells and release of mediators responsible for the clinical features of anaphylaxis (BMJ figure).
Rapid release of mediators in anaphylaxis causes the following events remembered by the mnemonic LESS:
Leakage (capilary) --> Urticaria, Angioedema, Laryngeal edema, Hypotension
Edema (mucosal) --> Laryngeal edema, Rhinitis, Wheezing
Smooth muscle contraction --> Wheezing, Abdominal pain
Shock
Increased vascular permeability (capilary leakage) can cause a shift of 50% of vascular volume to the extravascular space within 10 minutes, therefore leading to hypotension and shock. Epinephrine should be administered as early as possible to prevent this fluid shift and shock.
Etiology of anaphylaxis
Foods and insect venom are the 2 most common causes of anaphylaxis. Allergen immunotherapy (desensitization) may also induce anaphylaxis. A total of 46 deaths due to immunotherapy and skin testing were reported from 1945-1987.
Food ingestion is the cause of anaphylaxis in 36% of cases; a medication, allergy immunotherapy, or a diagnostic agent is the cause in 17% of cases; and insect stings are the cause in 15% of cases, 32% are idiopathic.
The common causes of anaphylaxis are remembered by the mneminic FIDL:
Foods - tree nuts, shellfish, 36%
Insect stings - Hymenoptera (bee and wasp), 15%
Drugs - beta-lactams, NSAIDs, 17%
Latex rubber
Anaphylaxis to penicillin (PCN) occurs in 1-5 cases per 10,000 patient treatment courses, with fatalities in 1 case per 50,000-100,000 courses. Insect stings cause 25-50 deaths per year in the U.S.
The largest study of childhood anaphylaxis (as of 2008) included 117 children. Home was the most common setting (48%) and food (85%) the most common trigger. The median age of presentation was 2.4 years. Peanut (18%) and cashew nut (13%) were the most common cause of anaphylaxis.
The 8 top allergens which account for 90 % of all food allergies are remembered by the mnemonic TEMPS WFS:
Tree nuts (almonds, cashews, walnuts)
Egg white (not egg yolk)
Milk
Peanuts
Shellfish (crab, lobster, shrimp)
Wheat
Fish (bass, cod, flounder)
Soy
The most common drugs causing anaphylaxis can be remembered by the mnemonic AAA CAN
Antibiotics (especially penicillin)
Anesthetic drugs, IV
ASA (aspirin)
Contrast media for radiologic studies, IV
Analgesic opioids
NSAIDs
Risk factors for anaphylaxis due to immunotherapy can be remembered by the mnemonic OH BEA:
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Clinical Features of anaphylaxis
The clinical features of anaphylaxis can be remembered by the mnemonic S ECG:
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 25%
Skin: Eythema, Pruritus, Urticaria, Angioedema.
Respiratory: Laryngeal edema, Wheezing, Rhinitis, Conjunctivitis, Itching of palate or external auditory meatus.
Cardiovascular: Palpitations, Sense of impending doom, Fainting, lightheadedness, Collapse, Loss of consciousness.
GI and oral: N/V/D, abdominal pain.
Specific features will often depend on route of allergen entry, for example, insect stings, intravenous drugs can cause cardiovascular problems, especially hypotension and shock. Foods which are absorbed transmucosally can cause lip, facial, and laryngeal edema.
Typically, symptom onset occurs within minutes after exposure and progression is rapid.
Latex rubber anaphylaxis is somewhat unusual because it develops more slowly (30 minutes) as the allergen has to be absorbed through the skin or mucosa.
Diagnosis of anaphylaxis
Anaphylaxis is a clinical diagnosis based on the history of acute exposure to an allergen followed by the typical systemic manifestations. Laboratory studies are not usually required.
Laboratory tests
- Histamine rises within 5-10 minutes and peaks at 30-60 minutes
- Tryptase peaks at 60-90 minutes and persist for 6 hours
- 24-hour urinary histamine metabolites are increased for up to 24 hours
Serum tryptase levels may not be reliable in food-induced anaphylaxis.
Serum tryptase levels may not be reliable in food-induced anaphylaxis.
Platelet-Activating Factor (PAF) may become the "BNP" of anaphylaxis in the future -- a laboratory test which helps in diagnosis. The analogy between PAF and BNP also comes from the fact that both tests help stratify the severity of the disease. The higher then BNP, the more severe the CHF exacerbation is. The same rule applies to PAF.
According to a study published in the NEJM, serum PAF levels were directly correlated with the severity of anaphylaxis. The proportion of subjects with elevated PAF levels increased from 4% in the control groups to 20% in the group with grade 1 anaphylaxis, 71% in the group with grade 2 anaphylaxis, and 100% in the group with grade 3 anaphylaxis.
Management of anaphylaxis
A recent study in the Annals of Allergy, Asthma and Immunology reported on development reported on development of the acronym SAFE, a mnemonic to remind physicians of the 4 action steps for anaphylaxis treatment:
Seek support
Allergen identification and avoidance
Follow-up for specialty care
Epinephrine for emergencies
Drugs used for management of anaphylaxis are remembered by the mnemonic EASI:
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension.
First-line therapy for anaphylaxis is epineprhrine (adrenaline) administered I.M. and it should be given as soon as the condition is recognized. Supplementary therapies include IVF, nebulized bronchodilators, antihistamines and corticosteroids (mnemonic EASI).
Epinephrine should not be given IV except under special circumstances such as profound shock or during anaesthesia. Myocardial infarction has rarely been reported in association with the use of epinephrine. Beta-blockers may increase the severity of an anaphylactic reaction and may antagonize the effect of epinephrine. Use of beta-blockers is not a contraindication to administering epinephrine. Glucagon IM can be administered in patients who take beta-blockers and have developed anaphylaxis.
Bi-phasic anaphylactic reactions have been described but are rare. Administration of steroids should minimize the risk of late relapse. The new guidelines require the prescription of 2 doses of self-injectable epinephrine to all patients (EpiPen 2-Pak).
Table: Management of acute anaphylaxis in the healthcare setting (adapted from Kemp et al. 2008).
Immediate intervention
- Assessment of airway, breathing, circulation and adequacy of mentation
- Administer adrenaline intramuscularly every 5–15 min, in appropriate doses, as necessary, depending on the presenting signs and symptoms of anaphylaxis, to control signs and symptoms and prevent progression to more severe symptoms such as respiratory distress, hypotension, shock and unconsciousness. Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
- Possibly appropriate, subsequent measures depending on response to adrenaline:
- Place patient in recumbent position and elevate lower extremities
- Establish and maintain airway
- Administer oxygen
- Establish venous access
- Normal saline intravenously for fluid replacement
Specific measures to consider after epinephrine injections, where appropriate:
Consider adrenaline infusion
Consider H1 and H2 antihistamines
Consider nebulized β2 agonist (e.g. albuterol [salbutamol]) for bronchospasm resistant to epinephrine
Consider systemic corticosteroids
Consider vasopressor (e.g. dopamine)
Consider glucagon for patient taking β-blocker
Consider atropine for symptomatic bradycardia
Consider transportation to an emergency department or an intensive care facility
For cardiopulmonary arrest during anaphylaxis, high-dose epinephrine and prolonged resuscitation efforts are encouraged, if necessary
1. Avoid exposure.
2. Refer to an allergist. Allergy assessment is mandatory in all patients with a history of anaphylaxis to identify and avoid the allergen to prevent its recurrence.
3. Preloaded EpiPen syringes for self treatment of anaphylaxis. Self-injectable epinephrine (adrenaline) should be prescribed in most patients with a history of anaphylaxis. According to a study published in JACI, there were 1,5 million EpiPen prescriptions filled in 2004 with an average of 5.7 EpiPens prescribed per 1000 persons. Massachusetts had the highest number of prescriptions per 1000 persons (11.8), Hawaii had the lowest (2.7). Overall, New England states clearly lead the group with 8-12 EpiPens prescribed per 1000 persons, whereas the southern states had only 3. Authors suggest that the relative lack of sun exposure and vitamin D status may lead to higher incidence of anaphylaxis in the northern states which could explain this strong north-south "gradient."
Patients may be advised to wear a Medic-Alert bracelet with a warning regarding anaphylaxis towards a specific allergen.
References
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Anaphylaxis: Recent advances in assessment and treatment. JACI, Volume 124, Issue 4, Pages 625-636 (October 2009).
Published: 09/08/2007
Updated: 06/22/2012
Anaphylaxis: Recent advances in assessment and treatment. JACI, Volume 124, Issue 4, Pages 625-636 (October 2009).
What Is Anaphylaxis? David B.K. Golden, MD. Current Opinion in Allergy and Clinical Immunology, Medscape, 09/2007.
Hospitalizations for Anaphylaxis in Florida: Epidemiologic Analysis of a Population-Based Dataset. Int Arch Allergy Immunol. 2007 May 25;144(2):128-136
Clinical review: ABC of allergies, Anaphylaxis. Pamela W Ewan. BMJ 1998;316:1442-1445.
Will Platelet-Activating Factor (PAF) be the "BNP" of Anaphylaxis? Allergy Notes, 01/2008.
Anaphylaxis articles from Allergy Notes.
How to Use EpiPen (Epinephrine) Auto-Injector. Allergy Notes.
Position paper: Management of anaphylaxis in childhood. EAACI Task Force on Anaphylaxis in Children. Allergy. 2007 Jun 21.
Anaphylactic Shock Due to Bee Sting. V. Dimov. Allergy Cases.
Anaphylaxis. Allergy Society of South Africa.
Anaphylaxis. eMedicine, 2005.
Paediatric anaphylaxis: a 5 year retrospective review. de Silva IL, Mehr SS, Tey D, Tang ML. Allergy. 2008 Aug;63(8):1071-6.
Anaphylaxis: diagnosis and management. Simon G A Brown, Raymond J Mullins and Michael S Gold. MJA 2006; 185 (5): 283-289.
Anaphylaxis in the Emergency Department: A Paediatric Perspective. Medscape, 11/2008.
Hospitalizations for Anaphylaxis in Florida: Epidemiologic Analysis of a Population-Based Dataset. Int Arch Allergy Immunol. 2007 May 25;144(2):128-136
Clinical review: ABC of allergies, Anaphylaxis. Pamela W Ewan. BMJ 1998;316:1442-1445.
Will Platelet-Activating Factor (PAF) be the "BNP" of Anaphylaxis? Allergy Notes, 01/2008.
Anaphylaxis articles from Allergy Notes.
How to Use EpiPen (Epinephrine) Auto-Injector. Allergy Notes.
Position paper: Management of anaphylaxis in childhood. EAACI Task Force on Anaphylaxis in Children. Allergy. 2007 Jun 21.
Anaphylactic Shock Due to Bee Sting. V. Dimov. Allergy Cases.
Anaphylaxis. Allergy Society of South Africa.
Anaphylaxis. eMedicine, 2005.
Paediatric anaphylaxis: a 5 year retrospective review. de Silva IL, Mehr SS, Tey D, Tang ML. Allergy. 2008 Aug;63(8):1071-6.
Anaphylaxis: diagnosis and management. Simon G A Brown, Raymond J Mullins and Michael S Gold. MJA 2006; 185 (5): 283-289.
Anaphylaxis in the Emergency Department: A Paediatric Perspective. Medscape, 11/2008.
What are the ‘ideal’ features of an adrenaline (epinephrine) auto-injector in the treatment of anaphylaxis? http://goo.gl/lxCh
Figure: Design overview of currently available auto-injectors for emergency self-administration of adrenaline in the treatment of anaphylaxis.
Related reading
Medicine in Stamps: Charles Richet (1850–1935): discoverer of anaphylaxis
History of Allergy: 1902, Charles Richet and Paul Portier invented the word 'anaphylaxis'
History of Allergy: 1902, Charles Richet and Paul Portier invented the word 'anaphylaxis'
Published: 09/08/2007
Updated: 06/22/2012
Subscribe to:
Posts (Atom)