Author: V. Dimov, M.D., Allergist/Immunologist, Cleveland Clinic Florida
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Allergic shiners: Dark circles under the eyes are due to swelling and discoloration from congestion of small blood vessels beneath the skin in this area. This can give the appearance of having "gone a few rounds" on the playground. The symptoms of allergic rhinitis often produce a combination of gestures and facial features (listed below), particularly in children and teenagers.
Dennie-Morgan lines: Young children with nasal allergies or atopic dermatitis have characteristic Dennie-Morgan lines. These are crease-like wrinkles that form under the lower eyelid folds (double skin folds).
Allergic salute: This describes the way that many children use the palm of their hand to rub and raise the tip of their nose to relieve nasal itching and congestion (and possibly to wipe away some mucus).
Nasal crease: This is a line across the bridge of the nose usually the result - particularly in children - of rubbing the nose (allergic salute) to relieve nasal congestion and itching.
Mouth breathing: Nasal congestion can result in chronic mouth breathing, associated with the development of a high, arched palate, an elevated upper lip, and an overbite. Teenagers with allergic rhinitis might end up needing braces.
Allergic (adenoidal) face (long face syndrome): Nasal allergies may promote swelling of the adenoids (lymph tissue that lines the back of the throat and extends behind the nose), resulting in a tired and droopy appearance.
Postnasal drip: Children may experience a constant postnasal drip and repeated sore throats from allergic mucus building up and being discharged into the throat. Serious nasal allergies also reduce the sense of taste and smell.
References
What Are Allergic Shiners? ACAAI.
Spotting an allergic child. BBC.
Published: 02/16/2012
Updated: 04/12/2016
Showing posts with label Rhinitis. Show all posts
Showing posts with label Rhinitis. Show all posts
Rhinitis Action Plan
Editor: V. Dimov, M.D., Allergist/Immunologist, Assistant Professor at University of Chicago
The Rhinitis Action Plan is available here (adapted by Dr. Dimov).
The parameters was developed by the Joint Task Force on Practice Parameters, representing the American Academy of Allergy, Asthma & Immunology; the American College of Allergy, Asthma and Immunology; and the Joint Council of Allergy, Asthma and Immunology.
References
The diagnosis and management of rhinitis: An updated practice parameter. Journal of Allergy and Clinical Immunology Vol. 122, Issue 2, Supplement, Pages S1-S84, August 2008 (PDF).
Related reading
Allergic Rhinitis Action Plans. Grand River Allergy.
Published: 06/07/2011
Updated: 08/11/2012
The Rhinitis Action Plan is available here (adapted by Dr. Dimov).
The parameters was developed by the Joint Task Force on Practice Parameters, representing the American Academy of Allergy, Asthma & Immunology; the American College of Allergy, Asthma and Immunology; and the Joint Council of Allergy, Asthma and Immunology.
References
The diagnosis and management of rhinitis: An updated practice parameter. Journal of Allergy and Clinical Immunology Vol. 122, Issue 2, Supplement, Pages S1-S84, August 2008 (PDF).
Related reading
Allergic Rhinitis Action Plans. Grand River Allergy.
Published: 06/07/2011
Updated: 08/11/2012
Allergic Rhinitis
 Editor: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Editor: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of ChicagoInformation For Patients
How to use a nose spray (video)
How to use a saline sinus rinse (video)
Allergic shiners, Dennie's lines, Allergic salute, Nasal crease, Postnasal drip
Rhinitis
Allergy Shots (Immunoterapy)
Allergy Testing
Action plan for rhinitis
Indoor Allergens
Outdoor Allergens
Sinusitis
Rhinosinusitis: Saline sinus rinse recipe
Checklist for Sneeze-Free and Wheeze-Free Home
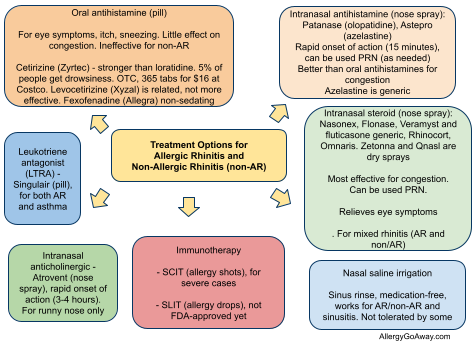
Treatment Options for Allergic Rhinitis (AR) and Non-Allergic Rhinitis (NAR) (click to enlarge the image).
Dust mite avoidance (click to enlarge the image).
What to expect when visiting an allergy clinic
Current allergy skin tests are virtually painless. This video by Dr. Bassett, a board-certified allergist from New York City, shows what to expect when visiting an allergy clinic for diagnosis and treatment:
Information For Doctors
Allergic Rhinitis: Teaching Cases
Allergic Rhinitis and Conjunctivitis
Cough Due to GERD in a Patient with Allergic Rhinitis
Treatment Devices for an Asthma and Allergic Rhinitis Patient with Arthritis and Stroke
Non-Allergic Rhinitis with Significant Nasal Discharge: How to Treat?
A female with asthma and allergic rhinitis who is trying to become pregnant: what medication changes may be needed?
More than a "runny nose" - allergic rhinitis and asthma
Anaphylactic reaction to subcutaneous immunotherapy: what to do?
How to treat rhinitis medicamentosa?
Allergic reaction after consumption of "meat-free chicken” (mycoprotein) by a patient with mold allergy
Almond allergy? No, it’s allergy to cockroach-contaminated chocolate-covered almonds
Related Reading
Allergic Rhinitis: Brief Review
Mind Maps: Allergic Rhinitis
Mnemonics: Allergic Rhinitis
How to use a nose spray - videos
Blog articles from AllergyNotes
Sinusitis: Brief Review
My Nasal Allergy Journal - free tools for patients by ACAAI
Unilateral Rhinorrhea in Allergic Rhinitis Due to... Cerebrospinal Fluid Leak. NEJM, 10/2009.
Nonallergic rhinitis, CCJM 2012 review.
Ocular Allergy: Allergic Conjunctivitis and Related Conditions, Brief Review
Mind Maps: Allergic Conjunctivitis
Mnemonics: Allergic Conjunctivitis
Cases of Allergic Conjunctivitis. Indiana University.
Image source: Wikipedia, Creative Commons license.
Published: 09/15/2007
Updated: 11/23/2012
Indoor Allergen Avoidance
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU

The word cloud of indoor allergens shows the frequency of term use in this article.
What is the strongest risk factor for asthma?
- sensitization to one or more of the major indoor allergens (dust mite, cat, dog, or cockroach, DCDC)
- accumulation of relevant allergens in the house
How the allergens change during the season: mnemonic TGR MI DC/DC ("a Tiger with an MI went to DC twice")
"There's spring time, where you have the tree pollen. Summer time, where you have the grass pollens. And then there's the fall time when you have the weed pollen.”
This sequence is remembered by the mnemonic TGR MI DC/DC ("a Tiger with an MI went to DC").
Pollen calendar: TGR MI DC/DC
Tree pollens
Grass pollens
Ragweed and weed pollen
Mold spores
Indoor allergens - DC/DC - Dog/Cat and Dust mite/Cockroach
Pollen-producing plants (weeds and trees) in Omaha, Nebraska
References:
Characteristics of allergic sensitization among asthmatic adults older than 55 years: results from the National Health Allergy Season Year Round. WTOC-TV Savannah.
Interactive Allergy Map by Greer Labs. Click your state to find region-specific, common airborne allergens there.
‘Botanical sexism’ blamed for making life miserable for allergy sufferers as male trees fill city skies with pollen http://goo.gl/cx5tH

Indoor allergens (click to enlarge the image).
The risk of house dust mite-sensitized children having current asthma doubles with every doubling of Der p I level.
Source: House dust mite allergens. A major risk factor for childhood asthma in Australia. Peat JK; Tovey E; Toelle BG; Haby MM; Gray EJ; Mahmic A; Woolcock AJ. Am J Respir Crit Care Med 1996 Jan;153(1):141-6.
Sensitivity to house dust mite and to cat dander are highly significant independent risk factors associated with the development of asthma, whereas grass sensitivity is not a significant independent risk factor for asthma.
Source: The relative risks of sensitivity to grass pollen, house dust mite and cat dander in the development of childhood asthma. Sears MR; Herbison GP; Holdaway MD; Hewitt CJ; Flannery EM; Silva PA. Clin Exp Allergy 1989 Jul;19(4):419-24.
Does a change in environment helps asthma symptoms?
Yes.
The level of bronchial hyperreactivity and the percentage of eosinophils in sputum samples were evaluated in a group of asthmatic children allergic to house dust mite before and after a 3-month period of antigen avoidance in an Alpine environment. Antigen avoidance significantly reduced the eosinophil phase of airway inflammation, along with bronchial hyperresponsiveness.
Source: Influence of allergen avoidance on the eosinophil phase of airway inflammation in children with allergic asthma. Piacentini GL; Martinati L; Mingoni S; Boner AL. J Allergy Clin Immunol 1996 May;97(5):1079-84.
Allergic patients should reduce allergen exposure in their houses as part of the management of asthma and allergic rhinitis.
Dust mites (Dermatophagoides pteronyssinus and D. farinae) (Der p1, Der f1)
_Lorryia_formosa_2_edit.jpg)
Yellow mite. Image source: Wikipedia, public domain.
Dust mites are arachnids that colonize bedding, sofas, carpets, and any woven material. Dust mites do not have eyes or antennae. They have 8 legs and a mouth-like appendage.
There are 2 different species:
- Dermatophagoides farinae is American HDM
- Dermatophagoides pteronyssinus is European HDM
The term arachnid is from the Greek word arachne, meaning spider, and also referring to the mythological figure Arachne.
Arachne was a great weaver. She boasted that her skill was greater than that of Athena the goddess of crafts, which resulted in a contest between her and the goddess. In the end the weaver won and the angry goddess turned Arachne into a spider.

Gustave Doré. Arachne (illustration to Dante's Purgatorio). Image source: Wikipedia, public domain
Dust mites do not bite and cannot be seen with a naked eye. The size of a HDM is 250-300 microns - 3 of them could fit inside the period at the end of this sentence.
Dust mites were first discovered by the inventor of the microscope, Anton van Leeuwenhoek. In 1694, Leeuwenhoek reported his discovery of microscopic "little animals" that live in dust.
What do mites drink?
They do not drink. Mites never drink but absorb humidity from the atmosphere, therefore they do not live optimally in dry environment. Dust mites are far less common in arid and high-altitude climates, such as the southwestern United States.
What do mites eat?
Mites feed on organic matter (shed human and animal skin particles) with the aid of fungal degradation.
"Dermatophagoides" means "skin eater."
Your mattress may contain between 100,000 and 10,000,000 dust mites.
During its 80-day lifespan, the average HDM produces about 1,000 fecal particles. A half teaspoon of dust contains 1,000 dust mites and 250,000 fecal particles.
Mite feces are a complex mixture of allergens:
- endotoxins
- enzymes
- mite and bacterial DNA
Der p 1 is a cysteine proteinase from feces of the HDM Dermatophagoides pteronyssinus.
Der p 1 elicits IgE antibody responses in patients with dust mite allergy. Der p 1 proteolytically cleaves the IL-2 receptor (CD25) on T cells which is involved in the homeostatic control of human IgE synthesis. Proteolytic activity of Der p 1 biases human CD4 and CD8 T cells towards a type 2 cytokine profile.
Source: Human T cell subset commitment determined by the intrinsic property of antigen: the proteolytic activity of the major mite allergen Der p 1 conditions T cells to produce more IL-4 and less IFN-gamma. Ghaemmaghami AM; Robins A; Gough L; Sewell HF; Shakib F. Eur J Immunol. 2001 Apr;31(4):1211-6.
House dust mite (HDM) feces are large and heavy (particles 6-10 micrometer in diameter) and are only transiently airborne.
Mite feces settle rapidly and are not detectable in the air within 15 minutes, therefore air filters have little role in controlling exposure.
Exposure to HDM occurs by close proximity to feces during time spent in bed, on the floor, or on upholstered furniture.
Measures to control HDM exposure

Dust mite allergen avoidance. The main allergen is in the dust mite feces. Use 3 control measures for 3-6 months to see an effect on the allergy symptoms (click to enlarge the image).

Dust Mite Control (click to enlarge the image).
Physical barriers
Covers:
- pillows
- mattresses
- box springs
- comforters
- furniture cushions
The simplest covers are made of plastic but they may be uncomfortable to use.
Gas permeable fabrics are an alternative to plastic covers.
Woven fabrics with a pore size of 6 microns block the passage of mites. Woven fabrics are preferable to non-woven materials which can retain high levels of allergen on the surface and lose integrity with repeated washing.
Benefit of bedding covers (as only intervention) on asthma control has not been well-documented
Minimizing reservoirs:
- pillow covers
- mattress covers
- washing bedding in hot water/dryer
- carpet removal
Bed covers reduce exposure to dust mite and improve adult atopic asthma http://buff.ly/1bSHY9g
Pet Allergens
Best solution: Do not to keep animals in the house.

Animal Dander Avoidance (click to enlarge the image).
What is the source of animal allergens?
Scales shed from the animal's skin (similar to human dander).
Restricting the animal to one part of the house is ineffective. For example, cat allergens are easily carried on clothing. Fewer than 50% of cat-allergic individuals report direct cat exposure (at home or elsewhere) (JACI, 2012).
Both cat (Fel d 1) and dog allergens (Can f 1) are small in size (different from HDM) and remain airborne for extended periods.
Many pet owner refuse to give away their animals. In this all too common scenario, allergen control can be attempted but is not very effective.
Even when a cat is removed from the house, allergens persist for weeks to months.
This explains why when a cat-allergic patient moves into a home in which a cat was previously living, he/she may have more symptoms.
Cat allergen is transferred on clothing and can be detected in schools and houses without a cat.
HEPA Air filters to reduce the concentration of airborne animal allergens
Unclear effect. Aggressive cleaning with HEPA filter vacuum may help.
- remove of existing mold
- decrease humidity below 50%
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU

The word cloud of indoor allergens shows the frequency of term use in this article.
What is the strongest risk factor for asthma?
- sensitization to one or more of the major indoor allergens (dust mite, cat, dog, or cockroach, DCDC)
- accumulation of relevant allergens in the house
How the allergens change during the season: mnemonic TGR MI DC/DC ("a Tiger with an MI went to DC twice")
"There's spring time, where you have the tree pollen. Summer time, where you have the grass pollens. And then there's the fall time when you have the weed pollen.”
This sequence is remembered by the mnemonic TGR MI DC/DC ("a Tiger with an MI went to DC").
Pollen calendar: TGR MI DC/DC
Tree pollens
Grass pollens
Ragweed and weed pollen
Mold spores
Indoor allergens - DC/DC - Dog/Cat and Dust mite/Cockroach
Pollen-producing plants (weeds and trees) in Omaha, Nebraska
References:
Characteristics of allergic sensitization among asthmatic adults older than 55 years: results from the National Health Allergy Season Year Round. WTOC-TV Savannah.
Interactive Allergy Map by Greer Labs. Click your state to find region-specific, common airborne allergens there.
‘Botanical sexism’ blamed for making life miserable for allergy sufferers as male trees fill city skies with pollen http://goo.gl/cx5tH

Indoor allergens (click to enlarge the image).
The risk of house dust mite-sensitized children having current asthma doubles with every doubling of Der p I level.
Source: House dust mite allergens. A major risk factor for childhood asthma in Australia. Peat JK; Tovey E; Toelle BG; Haby MM; Gray EJ; Mahmic A; Woolcock AJ. Am J Respir Crit Care Med 1996 Jan;153(1):141-6.
Sensitivity to house dust mite and to cat dander are highly significant independent risk factors associated with the development of asthma, whereas grass sensitivity is not a significant independent risk factor for asthma.
Source: The relative risks of sensitivity to grass pollen, house dust mite and cat dander in the development of childhood asthma. Sears MR; Herbison GP; Holdaway MD; Hewitt CJ; Flannery EM; Silva PA. Clin Exp Allergy 1989 Jul;19(4):419-24.
Does a change in environment helps asthma symptoms?
Yes.
The level of bronchial hyperreactivity and the percentage of eosinophils in sputum samples were evaluated in a group of asthmatic children allergic to house dust mite before and after a 3-month period of antigen avoidance in an Alpine environment. Antigen avoidance significantly reduced the eosinophil phase of airway inflammation, along with bronchial hyperresponsiveness.
Source: Influence of allergen avoidance on the eosinophil phase of airway inflammation in children with allergic asthma. Piacentini GL; Martinati L; Mingoni S; Boner AL. J Allergy Clin Immunol 1996 May;97(5):1079-84.
Allergic patients should reduce allergen exposure in their houses as part of the management of asthma and allergic rhinitis.
Dust mites (Dermatophagoides pteronyssinus and D. farinae) (Der p1, Der f1)
_Lorryia_formosa_2_edit.jpg)
Yellow mite. Image source: Wikipedia, public domain.
Dust mites are arachnids that colonize bedding, sofas, carpets, and any woven material. Dust mites do not have eyes or antennae. They have 8 legs and a mouth-like appendage.
There are 2 different species:
- Dermatophagoides farinae is American HDM
- Dermatophagoides pteronyssinus is European HDM
The term arachnid is from the Greek word arachne, meaning spider, and also referring to the mythological figure Arachne.
Arachne was a great weaver. She boasted that her skill was greater than that of Athena the goddess of crafts, which resulted in a contest between her and the goddess. In the end the weaver won and the angry goddess turned Arachne into a spider.

Gustave Doré. Arachne (illustration to Dante's Purgatorio). Image source: Wikipedia, public domain
Dust mites do not bite and cannot be seen with a naked eye. The size of a HDM is 250-300 microns - 3 of them could fit inside the period at the end of this sentence.
Dust mites were first discovered by the inventor of the microscope, Anton van Leeuwenhoek. In 1694, Leeuwenhoek reported his discovery of microscopic "little animals" that live in dust.
What do mites drink?
They do not drink. Mites never drink but absorb humidity from the atmosphere, therefore they do not live optimally in dry environment. Dust mites are far less common in arid and high-altitude climates, such as the southwestern United States.
What do mites eat?
Mites feed on organic matter (shed human and animal skin particles) with the aid of fungal degradation.
"Dermatophagoides" means "skin eater."
Your mattress may contain between 100,000 and 10,000,000 dust mites.
During its 80-day lifespan, the average HDM produces about 1,000 fecal particles. A half teaspoon of dust contains 1,000 dust mites and 250,000 fecal particles.
Mite feces are a complex mixture of allergens:
- endotoxins
- enzymes
- mite and bacterial DNA
Der p 1 is a cysteine proteinase from feces of the HDM Dermatophagoides pteronyssinus.
Der p 1 elicits IgE antibody responses in patients with dust mite allergy. Der p 1 proteolytically cleaves the IL-2 receptor (CD25) on T cells which is involved in the homeostatic control of human IgE synthesis. Proteolytic activity of Der p 1 biases human CD4 and CD8 T cells towards a type 2 cytokine profile.
Source: Human T cell subset commitment determined by the intrinsic property of antigen: the proteolytic activity of the major mite allergen Der p 1 conditions T cells to produce more IL-4 and less IFN-gamma. Ghaemmaghami AM; Robins A; Gough L; Sewell HF; Shakib F. Eur J Immunol. 2001 Apr;31(4):1211-6.
House dust mite (HDM) feces are large and heavy (particles 6-10 micrometer in diameter) and are only transiently airborne.
Mite feces settle rapidly and are not detectable in the air within 15 minutes, therefore air filters have little role in controlling exposure.
Exposure to HDM occurs by close proximity to feces during time spent in bed, on the floor, or on upholstered furniture.
Measures to control HDM exposure
Dust mite allergen avoidance. The main allergen is in the dust mite feces. Use 3 control measures for 3-6 months to see an effect on the allergy symptoms (click to enlarge the image).

Dust Mite Control (click to enlarge the image).
Physical barriers
Covers:
- pillows
- mattresses
- box springs
- comforters
- furniture cushions
The simplest covers are made of plastic but they may be uncomfortable to use.
Gas permeable fabrics are an alternative to plastic covers.
Woven fabrics with a pore size of 6 microns block the passage of mites. Woven fabrics are preferable to non-woven materials which can retain high levels of allergen on the surface and lose integrity with repeated washing.
Benefit of bedding covers (as only intervention) on asthma control has not been well-documented
Minimizing reservoirs:
- fabric and carpets
- upholstery and drapes
Remove carpets, upholstered furniture and drapes.
Vacuuming floors using a high-efficiency particular air (HEPA) filter.
Remove stuffed toys from bedroom.
Decrease humidity to below 50%
Decreasing humidity to below 50% reduces mite growth.
Best method: air conditioning in a humid climate.
Do not use humidifiers. Use dehumidifiers. Use saline nasal spray for dry nasal passages.
Upper floors are less humid. Patients allergic to HDM have less symptoms on 2nd floor.
Lower floor carpets often remain damp and become a rich source of bacterial, fungal, and dust mite allergens
Upper floor apartments have much less humidity than houses and 10-times less mite allergen.
Heat treatment of bedding
After washing, bedding should be dried in a dryer on a hot setting.
Insecticides are not useful.
Impact on asthma control was not consistent in studies due to confounding variables:
In 50% of the reported trials, dust mite avoidance failed -- the measures did not decrease allergen exposure for a significant period of time.
You need at least 3 methods for 3 months minimum:
Physical measures for 3-6 months:
- upholstery and drapes
Remove carpets, upholstered furniture and drapes.
Vacuuming floors using a high-efficiency particular air (HEPA) filter.
Remove stuffed toys from bedroom.
Decrease humidity to below 50%
Decreasing humidity to below 50% reduces mite growth.
Best method: air conditioning in a humid climate.
Do not use humidifiers. Use dehumidifiers. Use saline nasal spray for dry nasal passages.
Upper floors are less humid. Patients allergic to HDM have less symptoms on 2nd floor.
Lower floor carpets often remain damp and become a rich source of bacterial, fungal, and dust mite allergens
Upper floor apartments have much less humidity than houses and 10-times less mite allergen.
Heat treatment of bedding
After washing, bedding should be dried in a dryer on a hot setting.
Insecticides are not useful.
Impact on asthma control was not consistent in studies due to confounding variables:
In 50% of the reported trials, dust mite avoidance failed -- the measures did not decrease allergen exposure for a significant period of time.
You need at least 3 methods for 3 months minimum:
Physical measures for 3-6 months:
- pillow covers
- mattress covers
- washing bedding in hot water/dryer
- carpet removal
Bed covers reduce exposure to dust mite and improve adult atopic asthma http://buff.ly/1bSHY9g
Pet Allergens
Best solution: Do not to keep animals in the house.

Animal Dander Avoidance (click to enlarge the image).
What is the source of animal allergens?
Scales shed from the animal's skin (similar to human dander).
Restricting the animal to one part of the house is ineffective. For example, cat allergens are easily carried on clothing. Fewer than 50% of cat-allergic individuals report direct cat exposure (at home or elsewhere) (JACI, 2012).
Both cat (Fel d 1) and dog allergens (Can f 1) are small in size (different from HDM) and remain airborne for extended periods.
Many pet owner refuse to give away their animals. In this all too common scenario, allergen control can be attempted but is not very effective.
Even when a cat is removed from the house, allergens persist for weeks to months.
This explains why when a cat-allergic patient moves into a home in which a cat was previously living, he/she may have more symptoms.
Cat allergen is transferred on clothing and can be detected in schools and houses without a cat.
HEPA Air filters to reduce the concentration of airborne animal allergens
Unclear effect. Aggressive cleaning with HEPA filter vacuum may help.
In a 2001 Pediatrics study, HEPA Air Cleaners Were Not Very Effective For Decreasing Visits and Asthma Symptoms in Children Exposed to Tobacco Smoke.
Bathing pets
Washing cats weekly or less often does not improve symptoms. In any case, cat allergen in the air returns to pre-bath levels in 24 hours.
Washing dogs twice weekly may be helpful.
"Hypoallergenic cat"
Majority of people with cat allergy are sensitized to the Fel d 1 protein. A "hypoallergenic cat" ($4000 per cat) was developed (Allerca®) by breeding cats that were deficient in Fel d 1.
Initial studies showed fewer symptoms but allergen measurements were not published.
Rodents (mice and rats) (MUP)

Wood mouse, Apodemus sylvaticus. Image source: Wikipedia, public domain.
Rodents produce urinary proteins that are allergenic - mouse urinary protein (MUP).
Allergy to rodents in the workplace is an occupational health problem affecting research, pharmaceutical and toxicological sectors (Allergy to rodents: an update. Clin Exp Allergy. 2010 Sep. http://goo.gl/od2p). Mouse allergens are detectable in nearly all inner-city homes and in 75% of suburban homes. Allergen levels in inner-city homes are 100-1000-fold higher.
Exposure of infants to mouse allergens has been associated with the development of asthma, independent of other factors.
Control measures: extermination.
Cockroach (Bla g 1-4, Per a 1)

Female Blatella germanica with ootheca. Image source: Wikipedia, public domain.
Control measures: multiple baited traps with poison.
HEPA Air filtration is not helpful because the allergen settles quickly and does not remain airborne (similar to HDM).
Reducing exposure to cockroach allergen alone is unsuccessful because patients living in poor conditions are exposed to high levels of multiple allergens.
A combined strategy which reduces exposure to cockroach, mite and fungi is more successful.
Exposure to cockroach is linked to high shrimp IgE with questionable clinical reactivity - food challenge is needed for diagnosis (JACI, 2011).
Asian ladybugs (Harmonia axyridis)
Asian ladybugs were imported to the U.S. to control plant lice (aphids).

Asian Ladybug. Image source: Wikipedia, Creative Commons Attribution ShareAlike 2.5, Bruce Marlin, http://www.cirrusimage.com/beetles_multicolored_Asian_ladybird.htm

Aphids (plant lice). Image source: Wikipedia, GNU Free Documentation License.
It was anticipated that the insects would not survive the winter but they did by invading houses.
Asian ladybugs may cause seasonal indoor symptoms - chronic cough, rhinitis, and asthma.
Ladybug hemolymph is the primary source of allergens - Har a 1 and Har a 2. 'Reflex bleeding' from tibiofemoral joints (for communication and during alarm) disperses these allergens. Specific IgE immunoassays are not yet available.
Control measures:
- treatment of the outside of a house with pyrethroid before the cold weather
- move to a tightly-built house or into an urban area
Indoor molds

Moldy nectarines that were in a refrigerator. Image source: Wikipedia, GNU Free Documentation License.
Indoor molds affect homes with high humidity.
The 4 common allergenic molds include AAHP (Alternaria, Aspergillus, Hormodendrum, Penicillium).
Indoor mold remediation is beneficial in patients with asthma and visible home mold growth regardless of patient's sensitivity to the 4 common allergenic molds (AAHP) by skin prick testing. Medication use decreased 41% in the intervention group, and increased 17% in the control patients.
Why patients not sensitized to the 4 tested molds (AAHP) benefit?
Because of decrease in mycotoxins and volatile irritants released by growing molds.
Control measures:
Bathing pets
Washing cats weekly or less often does not improve symptoms. In any case, cat allergen in the air returns to pre-bath levels in 24 hours.
Washing dogs twice weekly may be helpful.
"Hypoallergenic cat"
Majority of people with cat allergy are sensitized to the Fel d 1 protein. A "hypoallergenic cat" ($4000 per cat) was developed (Allerca®) by breeding cats that were deficient in Fel d 1.
Initial studies showed fewer symptoms but allergen measurements were not published.
Rodents (mice and rats) (MUP)

Wood mouse, Apodemus sylvaticus. Image source: Wikipedia, public domain.
Rodents produce urinary proteins that are allergenic - mouse urinary protein (MUP).
Allergy to rodents in the workplace is an occupational health problem affecting research, pharmaceutical and toxicological sectors (Allergy to rodents: an update. Clin Exp Allergy. 2010 Sep. http://goo.gl/od2p). Mouse allergens are detectable in nearly all inner-city homes and in 75% of suburban homes. Allergen levels in inner-city homes are 100-1000-fold higher.
Exposure of infants to mouse allergens has been associated with the development of asthma, independent of other factors.
Control measures: extermination.
Cockroach (Bla g 1-4, Per a 1)

Female Blatella germanica with ootheca. Image source: Wikipedia, public domain.
Control measures: multiple baited traps with poison.
HEPA Air filtration is not helpful because the allergen settles quickly and does not remain airborne (similar to HDM).
Reducing exposure to cockroach allergen alone is unsuccessful because patients living in poor conditions are exposed to high levels of multiple allergens.
A combined strategy which reduces exposure to cockroach, mite and fungi is more successful.
Exposure to cockroach is linked to high shrimp IgE with questionable clinical reactivity - food challenge is needed for diagnosis (JACI, 2011).
Asian ladybugs (Harmonia axyridis)
Asian ladybugs were imported to the U.S. to control plant lice (aphids).

Asian Ladybug. Image source: Wikipedia, Creative Commons Attribution ShareAlike 2.5, Bruce Marlin, http://www.cirrusimage.com/beetles_multicolored_Asian_ladybird.htm

Aphids (plant lice). Image source: Wikipedia, GNU Free Documentation License.
It was anticipated that the insects would not survive the winter but they did by invading houses.
Asian ladybugs may cause seasonal indoor symptoms - chronic cough, rhinitis, and asthma.
Ladybug hemolymph is the primary source of allergens - Har a 1 and Har a 2. 'Reflex bleeding' from tibiofemoral joints (for communication and during alarm) disperses these allergens. Specific IgE immunoassays are not yet available.
Control measures:
- treatment of the outside of a house with pyrethroid before the cold weather
- move to a tightly-built house or into an urban area
Indoor molds

Moldy nectarines that were in a refrigerator. Image source: Wikipedia, GNU Free Documentation License.
Indoor molds affect homes with high humidity.
The 4 common allergenic molds include AAHP (Alternaria, Aspergillus, Hormodendrum, Penicillium).
Indoor mold remediation is beneficial in patients with asthma and visible home mold growth regardless of patient's sensitivity to the 4 common allergenic molds (AAHP) by skin prick testing. Medication use decreased 41% in the intervention group, and increased 17% in the control patients.
Why patients not sensitized to the 4 tested molds (AAHP) benefit?
Because of decrease in mycotoxins and volatile irritants released by growing molds.
Control measures:
- remove of existing mold
- decrease humidity below 50%
Regarding the mold/asthma link, certain findings have been found consistently: 1. the mold has to be visible, 2. the mold has to be in the room where they live, 3. the patient does not have to be allergic to mold to have symptoms because the some molds release irritant volatile compounds in the air.
Outdoor pollens: Prevention
Keep windows closed
Use air conditioning at home and in the car
Minimize early morning activity (5-10 AM) when pollen is usually emitted
Stay indoors when humidity is high or on windy days
Shower and change clothes following outdoor activity to remove pollen from hair, skin, clothing
Avoid locations likely to have high levels of pollens: fields, woods, etc.
Do not mow lawn or rake leaves
References
Indoor Allergen Avoidance. Thomas A.E. Platts-Mills, MD, PhD. UpToDate, 16.2.
A Closer Look at Dust Mites. Achoo Allergy.
Related Reading
CNN: What to do if you're allergic to your pet http://bit.ly/Eu74n
Outdoor pollens: Prevention
Keep windows closed
Use air conditioning at home and in the car
Minimize early morning activity (5-10 AM) when pollen is usually emitted
Stay indoors when humidity is high or on windy days
Shower and change clothes following outdoor activity to remove pollen from hair, skin, clothing
Avoid locations likely to have high levels of pollens: fields, woods, etc.
Do not mow lawn or rake leaves
References
Indoor Allergen Avoidance. Thomas A.E. Platts-Mills, MD, PhD. UpToDate, 16.2.
A Closer Look at Dust Mites. Achoo Allergy.
Related Reading
CNN: What to do if you're allergic to your pet http://bit.ly/Eu74n
6 common indoor allergy triggers and how to avoid them. South Florida Sun-Sentinel, 2010.
Peptide immunotherapy vaccine for cat allergy - effective as a single dose in a German study http://goo.gl/4l4Vq
PowerPoint Presentations
Related:
How Select the Right Dehumidifier | Achoo! Blog http://buff.ly/2bPtmeX
Published: 11/01/2008
Updated: 04/15/2012
PowerPoint Presentations
Related:
How Select the Right Dehumidifier | Achoo! Blog http://buff.ly/2bPtmeX
Published: 11/01/2008
Updated: 04/15/2012
Cough Due to GERD in a Patient with Allergic Rhinitis
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 37-year-old female with allergic rhinitis on immunotherapy comes to the allergy clinic with symptoms of dry cough and heartburn for 3 weeks. She has had this type of cough off and on for the last 2 years. The patient was treated with Prilosec 1.5 years ago with good effect but she stopped the medication after 4 months due to "bloating." She would like to receive her immunotherapy shot today.
Past medical history (PMH)
Alelrgic rhinitis.
Medications
Flonase (fluticasone), Zyrtec (cetirizine).
Skin testing
Two years ago.
Pulmonary function tests (PFTs)
Normal, 1 year ago
Immunotherapy
Started 5 months ago, last dose was 4 weeks ago. Grass and tree extracts were used.
Pets
Dog and cat, the family also has horses and chicken.
Physical examination
Normal.
Spirometry today
Normal.
What is the reason for the cough?
Most likely GERD.
What would you do?
The patient was prescribed Nexium and advised to return to the clinic in 2 weeks.
Would you give the scheduled immunotherapy injection today?
It is generally advisable to postpone the administration of the immunotherapy injection until acute symptoms resolve. If the patient's symptoms worsen after the injection, it would be unclear what the cause was: GERD or anaphylaxis.
Which animal is "worse" for pollen-allergic patients - cat or dog?
A typical cat spends most of his/her life indoors and although cat hair has a higher allergic potential than dog hair, cats are less important than dogs for patients with pollen-related allergies. Many dogs, on the other hand, roam outside every day and get back home with "a suit of tree, grass, weed and mold."
Final diagnosis
GERD-related cough.

Differential diagnosis of cough, a simple mnemonic is GREAT BAD CAT TOM. Click here to enlarge the image: (GERD (reflux), Laryngopharyngeal Reflux (LPR), Rhinitis (both allergic and non-allergic) with post-nasal drip (upper airway cough syndrome), Embolism, e.g. PE in adults, Asthma, TB (tuberculosis), Bronchitis, pneumonia, pertussis, Aspiration, e.g foreign body in children, Drugs, e.g. ACE inhibitor, CF in children, Cardiogenic, e.g. mitral stenosis in adults, Achalasia in adults, Thyroid enlargement, e.g. goiter, "Thoughts" (psychogenic), Other causes, Malignancy, e.g. lung cancer in adults).
What did we learn from this case?
GERD is a common cause of cough in patients with allergy in the absence of asthma. It is prudent to await the resolution of acute symptoms before immunotherapy is resumed.
Treatment Options for Allergic Rhinitis (click to enlarge the image).
Published: 07/03/2008
Updated: 01/11/2012
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 37-year-old female with allergic rhinitis on immunotherapy comes to the allergy clinic with symptoms of dry cough and heartburn for 3 weeks. She has had this type of cough off and on for the last 2 years. The patient was treated with Prilosec 1.5 years ago with good effect but she stopped the medication after 4 months due to "bloating." She would like to receive her immunotherapy shot today.
Past medical history (PMH)
Alelrgic rhinitis.
Medications
Flonase (fluticasone), Zyrtec (cetirizine).
Skin testing
Two years ago.
Pulmonary function tests (PFTs)
Normal, 1 year ago
Immunotherapy
Started 5 months ago, last dose was 4 weeks ago. Grass and tree extracts were used.
Pets
Dog and cat, the family also has horses and chicken.
Physical examination
Normal.
Spirometry today
Normal.
What is the reason for the cough?
Most likely GERD.
What would you do?
The patient was prescribed Nexium and advised to return to the clinic in 2 weeks.
Would you give the scheduled immunotherapy injection today?
It is generally advisable to postpone the administration of the immunotherapy injection until acute symptoms resolve. If the patient's symptoms worsen after the injection, it would be unclear what the cause was: GERD or anaphylaxis.
Which animal is "worse" for pollen-allergic patients - cat or dog?
A typical cat spends most of his/her life indoors and although cat hair has a higher allergic potential than dog hair, cats are less important than dogs for patients with pollen-related allergies. Many dogs, on the other hand, roam outside every day and get back home with "a suit of tree, grass, weed and mold."
Final diagnosis
GERD-related cough.
Differential diagnosis of cough, a simple mnemonic is GREAT BAD CAT TOM. Click here to enlarge the image: (GERD (reflux), Laryngopharyngeal Reflux (LPR), Rhinitis (both allergic and non-allergic) with post-nasal drip (upper airway cough syndrome), Embolism, e.g. PE in adults, Asthma, TB (tuberculosis), Bronchitis, pneumonia, pertussis, Aspiration, e.g foreign body in children, Drugs, e.g. ACE inhibitor, CF in children, Cardiogenic, e.g. mitral stenosis in adults, Achalasia in adults, Thyroid enlargement, e.g. goiter, "Thoughts" (psychogenic), Other causes, Malignancy, e.g. lung cancer in adults).
What did we learn from this case?
GERD is a common cause of cough in patients with allergy in the absence of asthma. It is prudent to await the resolution of acute symptoms before immunotherapy is resumed.
Treatment Options for Allergic Rhinitis (click to enlarge the image).
Related reading
In patients with asthma and chronic productive cough, polymorphonuclear (PMN) neutrophil leukocytes in sputum suggest:
(A) infection
(B) GERD
(C) presence of a foreign body
(D) exercise-induced asthma
(E) extrinsic asthma
Correct answers: A, B, C
PPIs Not Recommended for Routine Treatment of Adult Asthma - in patients with "silent" GERD. Medscape, 2011.
Insufficient evidence to recommend empirical use of PPIs for routine treatment of asthma. Arch Intern Med. 2011;171(7):620-629.
Updated: 01/11/2012
Anaphylactic reaction to subcutaneous immunotherapy: what to do?
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 31-year-old Caucasian male has been on subcutaneous immunotherapy for allergic rhinitis for 3 months. The subcutaneous immunotherapy (SCIT) consists of 3 injections with extracts of grasses, trees, weeds (vial A), dust mite, molds (vial B), cat and ragweed (vial C). His maintenance dose goal is 0.5 ml.
The SCIT dose was gradually increased with weekly injections and the dose he received last week was 0.3 ml. The patient reports large local reactions which started at the level of 0.1 ml and increased progressively as the dose increased to 0.2 ml.
During the last visit, the size of the local reaction was 30 x 30 mm in terms of swelling. He has no history of prior systemic reactions to SCIT.
Past medical history (PMH)
Allergic rhinitis. He has a remote history of mild asthma, which has been asymptomatic for years and he used only occasionally a prn albuterol inhaler in the remote past.
Medications
Benadryl PRN, Flonase (fluticasone) nasal spray daily
What happened?
The patient received three injections of immunotherapy today at 10:50 and within two to three minutes of the injection, he started to complain of feeling that his throat was closing, dry cough and itchy eyes. He was evaluated immediately by the nurses and his allergist.
What is the most likely diagnosis?
He was found to have an anaphylactic reaction to the subcutaneous immunotherapy.
What treatment would you suggest?
He was given a dose of epineprine 0.3 mg IM at 10:51 and Alavert 10 mg po dissolvable tablet at 10:52. At that time, his blood pressure was 140/55, heart rate was 112, and his pulse-oximetry was 93% on room air.
At 11:00, he was given 40 mg of prednisone po x 1.
What happened next?
The patient reported that his throat sensation was better; however, his pulse-oximetry was noted to be in the range of 90% and on physical examination, he developed diffuse bilateral expiratory wheezing. The physical examination was also remarkable for conjunctival injection and development of swelling around the injection site on both arms with large, local reaction in the range of 8 to 9 cm on the left arm with wheals and satellite wheals around the injection sites.
What treatment would you suggest next?
He was treated with albuterol four puffs at 11:15. At 11:20, he reported improvement in his throat sensation and shortness of breath. His pulse-oximetry was 96%; blood pressure was 130/80.
At 11:30, the patient reportedly returned to baseline in terms of his symptoms. On physical examination, he had no more wheezing.
He was given a prescription for prednisone 40 mg po daily for three days and loratadine 10 mg po daily for seven days.
How would you change the immunotherapy prescription?
His dose of immunotherapy was returned to the dose two steps before the current one, which was 0.1 ml and he is to stay on this dose for two months.
The patient was discharged from the clinic at 12:50, two hours after the event. He is on prednisone, which should prevent any symptoms of late reaction.
Final diagnosis
Anaphylactic reaction to subcutaneous immunotherapy
Summary

Anaphylaxis mind map diagram.
Allergen immunotherapy was introduced by Leonard Noon 100 years ago and is the only disease-modifying treatment for allergic individuals (Allergy, 2012).
During a retrospective chart review of 388 patients, the rate of systemic reactions during subcutaneous immunotherapy was 0.28% per injection and 7.4% per patient. It was concerning that 48% of the systemic reactions occurred more than 30 minutes after the injection and many of these reactions required epinephrine.
This study was unable to identify risk factors that predict the reactions. Gender, phase (build-up versus maintenance), asthma, angiotensin-converting enzyme inhibitors, beta-blockers, initial skin-prick test size, or allergen type did not increase the odds of a systemic reaction.
Skin prick testing (SPT) on beta-blockers was safe in 199 patients in a 2012 study (http://goo.gl/3vGSl). However, incidence of systemic reactions is 1:250 with SPT.
Mnemonics for anaphylaxis
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
References
Allergen immunotherapy safety: Characterizing systemic reactions and identifying risk factors. Rank, Mathew A.; Oslie, Corrine L.; Krogman, Jennifer L.; Park, Miguel A.; Li, James T. Allergy and Asthma Proceedings, Volume 29, Number 4, 7/8 2008 , pp. 400-405(6).
Evaluation of near-fatal reactions to allergen immunotherapy injections. Amin HS, Liss GM, Bernstein DI. J Allergy Clin Immunol. 2006 Jan;117(1):169-75.
Anaphylactic reactions during immunotherapy. Rezvani M, Bernstein DI. Immunol Allergy Clin North Am. 2007 May;27(2):295-307, viii.
Allergen immunotherapy: A practice parameter second update. JACI, 2007 (PDF).
Anaphylaxis: A Short Review
Rate of systemic reactions during subcutaneous immunotherapy: 0.28% per injection
Mnemonics: Anaphylaxis
Mind Maps: Anaphylaxis
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 31-year-old Caucasian male has been on subcutaneous immunotherapy for allergic rhinitis for 3 months. The subcutaneous immunotherapy (SCIT) consists of 3 injections with extracts of grasses, trees, weeds (vial A), dust mite, molds (vial B), cat and ragweed (vial C). His maintenance dose goal is 0.5 ml.
The SCIT dose was gradually increased with weekly injections and the dose he received last week was 0.3 ml. The patient reports large local reactions which started at the level of 0.1 ml and increased progressively as the dose increased to 0.2 ml.
During the last visit, the size of the local reaction was 30 x 30 mm in terms of swelling. He has no history of prior systemic reactions to SCIT.
Past medical history (PMH)
Allergic rhinitis. He has a remote history of mild asthma, which has been asymptomatic for years and he used only occasionally a prn albuterol inhaler in the remote past.
Medications
Benadryl PRN, Flonase (fluticasone) nasal spray daily
What happened?
The patient received three injections of immunotherapy today at 10:50 and within two to three minutes of the injection, he started to complain of feeling that his throat was closing, dry cough and itchy eyes. He was evaluated immediately by the nurses and his allergist.
What is the most likely diagnosis?
He was found to have an anaphylactic reaction to the subcutaneous immunotherapy.
What treatment would you suggest?
He was given a dose of epineprine 0.3 mg IM at 10:51 and Alavert 10 mg po dissolvable tablet at 10:52. At that time, his blood pressure was 140/55, heart rate was 112, and his pulse-oximetry was 93% on room air.
At 11:00, he was given 40 mg of prednisone po x 1.
What happened next?
The patient reported that his throat sensation was better; however, his pulse-oximetry was noted to be in the range of 90% and on physical examination, he developed diffuse bilateral expiratory wheezing. The physical examination was also remarkable for conjunctival injection and development of swelling around the injection site on both arms with large, local reaction in the range of 8 to 9 cm on the left arm with wheals and satellite wheals around the injection sites.
What treatment would you suggest next?
He was treated with albuterol four puffs at 11:15. At 11:20, he reported improvement in his throat sensation and shortness of breath. His pulse-oximetry was 96%; blood pressure was 130/80.
At 11:30, the patient reportedly returned to baseline in terms of his symptoms. On physical examination, he had no more wheezing.
He was given a prescription for prednisone 40 mg po daily for three days and loratadine 10 mg po daily for seven days.
How would you change the immunotherapy prescription?
His dose of immunotherapy was returned to the dose two steps before the current one, which was 0.1 ml and he is to stay on this dose for two months.
The patient was discharged from the clinic at 12:50, two hours after the event. He is on prednisone, which should prevent any symptoms of late reaction.
Final diagnosis
Anaphylactic reaction to subcutaneous immunotherapy
Summary

Anaphylaxis mind map diagram.
Allergen immunotherapy was introduced by Leonard Noon 100 years ago and is the only disease-modifying treatment for allergic individuals (Allergy, 2012).
During a retrospective chart review of 388 patients, the rate of systemic reactions during subcutaneous immunotherapy was 0.28% per injection and 7.4% per patient. It was concerning that 48% of the systemic reactions occurred more than 30 minutes after the injection and many of these reactions required epinephrine.
This study was unable to identify risk factors that predict the reactions. Gender, phase (build-up versus maintenance), asthma, angiotensin-converting enzyme inhibitors, beta-blockers, initial skin-prick test size, or allergen type did not increase the odds of a systemic reaction.
Skin prick testing (SPT) on beta-blockers was safe in 199 patients in a 2012 study (http://goo.gl/3vGSl). However, incidence of systemic reactions is 1:250 with SPT.
Mnemonics for anaphylaxis
Clinical features of anaphylaxis: S ECG
Skin, 90%
Expiratory wheezing and other respiratory symptoms, 70%
Cardiovascular, 40%
GI and oral, 24%
Risk factors for anaphylaxis due to immunotherapy include: OH BEA
Observation - insufficient, following injection
High allergen dose
Beta-blockers
Errors in administration
Asthma, poorly controlled
Drugs for acute management of anaphylaxis: EASI
Epinephrine IM
Antihistamines PO, IM
Steroids PO, IM, IV
Inhaled b2-agonists, if wheezing. IV fluids if hypotension
Epinephrine (adrenaline) is the first-line the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration. This should be given in the lateral aspect of the thigh by intramuscular injection. The dose can be repeated every 5 to 15 minutes, depending upon the response, for 3-4 doses. The same is true for children except the dose is 0.01 mg per kg (AAAAI Ask the Expert, 2012).
What are the 4 standardized allergen extracts?
(A) Dog
(B) Trees
(C) Cat
(D) Molds
(E) Dust Mite
(F) Grass
(G) Ragweed
The 4 standardized extracts are Cat, Dust Mite, Grass and Ragweed.
References
Allergen immunotherapy safety: Characterizing systemic reactions and identifying risk factors. Rank, Mathew A.; Oslie, Corrine L.; Krogman, Jennifer L.; Park, Miguel A.; Li, James T. Allergy and Asthma Proceedings, Volume 29, Number 4, 7/8 2008 , pp. 400-405(6).
Evaluation of near-fatal reactions to allergen immunotherapy injections. Amin HS, Liss GM, Bernstein DI. J Allergy Clin Immunol. 2006 Jan;117(1):169-75.
Anaphylactic reactions during immunotherapy. Rezvani M, Bernstein DI. Immunol Allergy Clin North Am. 2007 May;27(2):295-307, viii.
Allergen immunotherapy: A practice parameter second update. JACI, 2007 (PDF).
Anaphylaxis: A Short Review
Rate of systemic reactions during subcutaneous immunotherapy: 0.28% per injection
Mnemonics: Anaphylaxis
Mind Maps: Anaphylaxis
Anaphylaxis guidelines by World Allergy Organization. JACI, 2011.
Published: 02/12/2009
Updated: 06/12/2012
Published: 02/12/2009
Updated: 06/12/2012
Non-Allergic Rhinitis with Significant Nasal Discharge: How to Treat?
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 35-year-old African American male is referred to the allergy clinic for evaluation of allergic rhinitis for 4 years. He first developed nasal congestion, discharge, sneezing and itching 4 years ago when he moved from Florida to Alabama. He has taken Zyrtec-D (cetirizine, pseudoephedrine) daily during that period with partial relief and has occasionally used Flonase. The patient has never had allergy skin testing before. He was initially seen at the clinic last week while still taking Zyrtec (changed from Zyrtec-D by his insurance) and Amitriptyline, and the skin prick testing was postponed. He was asked to stop Zyrtec and Amitriptyline 5 days before the test and was prescribed Flonase (fluticasone).
Past medical history (PMH)
Oral antihistamines are ineffective for non-AR. Intranasal antihistamines however, are approved for vasomotor rhinitis (non-AR) which makes them a good option for patients with mixed rhinitis (AR/non-AR).
References
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
A 35-year-old African American male is referred to the allergy clinic for evaluation of allergic rhinitis for 4 years. He first developed nasal congestion, discharge, sneezing and itching 4 years ago when he moved from Florida to Alabama. He has taken Zyrtec-D (cetirizine, pseudoephedrine) daily during that period with partial relief and has occasionally used Flonase. The patient has never had allergy skin testing before. He was initially seen at the clinic last week while still taking Zyrtec (changed from Zyrtec-D by his insurance) and Amitriptyline, and the skin prick testing was postponed. He was asked to stop Zyrtec and Amitriptyline 5 days before the test and was prescribed Flonase (fluticasone).
Past medical history (PMH)
Rhinitis, migraine headache.
Medications
Medications
Zyrtec (cetirizine), amitriptyline (both stopped 5 days ago), Flonase (intranasal fluticasone)
Social history (SH)
Social history (SH)
Accountant. No tobacco use, no pets.
Physical examination
Stable vital signs (VSS). HEENT: Pale, boggy turbinates. Chest: CTA (B).
What diagnostic test would you suggest?
What diagnostic test would you suggest?
Skin prick testing.
Amitriptyline has an antihistamine effect, and both Amitriptyline and Zyrtec had to be stopped 5 days prior to testing.
The skin prick testing was negative for trees, grass, weeds, molds and indoor allergens (1-35 pricks). The histamine control was positive which indicated an adequate skin reaction. If the histamine control is negative in a patient on antihistamine, the reason could be that the patient is still taking the medication.

Skin test sheet. Image source: Dr. Stokes, Creighton University Division of Allergy & Immunology, used with permission (click to enlarge the image).

Diagram of skin prick testing (click to enlarge the image).
What is the most likely diagnosis?
Amitriptyline has an antihistamine effect, and both Amitriptyline and Zyrtec had to be stopped 5 days prior to testing.
The skin prick testing was negative for trees, grass, weeds, molds and indoor allergens (1-35 pricks). The histamine control was positive which indicated an adequate skin reaction. If the histamine control is negative in a patient on antihistamine, the reason could be that the patient is still taking the medication.

Skin test sheet. Image source: Dr. Stokes, Creighton University Division of Allergy & Immunology, used with permission (click to enlarge the image).

Diagram of skin prick testing (click to enlarge the image).
What is the most likely diagnosis?
Non-allergic rhinitis.
What questions would you ask to confirm the diagnosis of non-allergic rhinitis?
What questions would you ask to confirm the diagnosis of non-allergic rhinitis?
The patient was asked if he reacts to strong odors, perfumes, smoke and temperature changes. He reported nasal symptoms with strong odors and perfumes, predominantly manifested by increased nasal discharge.
Was there any seasonal variation in his nasal symptoms?
Was there any seasonal variation in his nasal symptoms?
No. Nasal discharge was persistent throughout the year.
Typically, allergic rhinitis is worse during the pollen season corresponding to the patient's allergies: spring for trees, summer for grass, fall for weeds, and year round for molds and indoor allergens.
Did he get worse after stopping Zyrtec (cetirizine)?
Typically, allergic rhinitis is worse during the pollen season corresponding to the patient's allergies: spring for trees, summer for grass, fall for weeds, and year round for molds and indoor allergens.
Did he get worse after stopping Zyrtec (cetirizine)?
No.
Typically, patients with allergic rhinitis report symptom worsening after stopping antihistimines. Zyrtec has no effect in patients with non-allergic rhinitis. Our patient reported a partial relief with Zyrtec-D because of the pseudoephedrine component rather than cetirizine.
How would you treat this patient with non-allergic rhinitis?
Typically, patients with allergic rhinitis report symptom worsening after stopping antihistimines. Zyrtec has no effect in patients with non-allergic rhinitis. Our patient reported a partial relief with Zyrtec-D because of the pseudoephedrine component rather than cetirizine.
How would you treat this patient with non-allergic rhinitis?
Flonase (fluticasone) should be continued.
Atrovent 0.03% nasal spray PRN bid was added since nasal discharge was the most bothersome symptom.
He was advised to use nasal saline rinses and to follow-up with us in 3 months. A CT scan of the sinuses was ordered to rule out an anatomical abnormality.
Final diagnosis
Atrovent 0.03% nasal spray PRN bid was added since nasal discharge was the most bothersome symptom.
He was advised to use nasal saline rinses and to follow-up with us in 3 months. A CT scan of the sinuses was ordered to rule out an anatomical abnormality.
Final diagnosis
Non-allergic rhinitis.
What did we learn from this case?
What did we learn from this case?
Intranasal anticholinergic (ipratropium) has a rapid onset of action (3-4 hours, similar to intranasal antihistamines) and can be used for for episodic rhinitis.
Ipratropium reduces rhinorrhea but is otherwise ineffective for congestion and other symptoms of AR.
Atrovent can cause extreme nasal dryness and therefore should be used PRN by most patients rather than continuously.

Treatment Options for Allergic Rhinitis (AR) and Non-Allergic Rhinitis (NAR) (click to enlarge the image).
Ipratropium reduces rhinorrhea but is otherwise ineffective for congestion and other symptoms of AR.
Atrovent can cause extreme nasal dryness and therefore should be used PRN by most patients rather than continuously.
Treatment Options for Allergic Rhinitis (AR) and Non-Allergic Rhinitis (NAR) (click to enlarge the image).
Oral antihistamines are ineffective for non-AR. Intranasal antihistamines however, are approved for vasomotor rhinitis (non-AR) which makes them a good option for patients with mixed rhinitis (AR/non-AR).
References
Guidelines Updated for Diagnosis and Treatment of Rhinitis. Laurie Barclay. Medscape.
The Diagnosis and Management of Rhinitis: An Updated Practice Parameter. The Journal of Allergy and Clinical Immunology, Volume 122, Issue 2, Supplement (August 2008).
Nonallergic rhinitis, CCJM 2012 review.
Image source: Wikipedia, a Creative Commons license.
Allergic Rhinitis: A Short Review
Mind Maps: Allergic Rhinitis
The Diagnosis and Management of Rhinitis: An Updated Practice Parameter. The Journal of Allergy and Clinical Immunology, Volume 122, Issue 2, Supplement (August 2008).
Nonallergic rhinitis, CCJM 2012 review.
Image source: Wikipedia, a Creative Commons license.
{kind=link}
Allergic Rhinitis: A Short Review
Mind Maps: Allergic Rhinitis
Got allergies? Maybe it's actually non-allergic rhinitis. USA Today, 2010.
"Allergic" Reactions in Adults May Be Vasomotor or Nonallergic Rhinitis. WSJ, 2011.
Management of recalcitrant nasal congestion in chronic nonallergic rhinitis: fluticasone, azelastine, and capsaicin. AAAAI Ask the Expert, 2011.
Published: 08/25/2008
Updated: 12/23/2012
Management of recalcitrant nasal congestion in chronic nonallergic rhinitis: fluticasone, azelastine, and capsaicin. AAAAI Ask the Expert, 2011.
Published: 08/25/2008
Updated: 12/23/2012
Adult Sinusitis: Brief Review
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Nasal physiology
Mucociliary clearance can be tested by placing saccharin on the inferior turbinate and timing the onset of sweet taste in the mouth. The normal range is 7-11 minutes.
There is normal asymmetry of nasal mucosa swelling, with one side of nose swollen as a result of dilatation of veins in the inferior turbinate and the other side "open" - 80% of the population exhibits a nasal cycle, with reciprocal changes in airflow over 1-2 hours.
Anatomy
Sinus is a Latin word for “fold” or “pocket”. Paranasal sinuses have an embryogenic origin from the nasal passage and are an integral component of the airway. Drainage pathways of the sinuses are complex and can be blocked during inflammation. Ostia are the sinus openings in the nasal cavity. They are 2-6 mm wide.
Sinusitis
Approximately 31-35 million Americans are affected by sinusitis every year (15% of the population).
Sinusitis of less than 4 weeks’ duration is considered acute. Chronic sinusitis persists for more than 4 weeks.
Recurrent sinusitis is defined as 4 or more episodes of sinusitis per year. Each episode lasting 7-10 days and no symptoms during intervening periods.
Acute Exacerbation of Chronic Sinusitis is the sudden worsening of chronic sinusitis that returns to baseline with treatment.
The term sinusitis is often interpreted as reflecting simply a bacterial sinus infection but the disease can have a significant allergic component.
Sinusitis is mostly preceded by rhinitis and is rarely found without rhinitis.
The 1997 Rhinosinusitis Task Force thus proposed the term Rhinosinusitis instead of Sinusitis (reiterated in 2007 guidelines).
Acute Sinusitis
Symptoms for up to 4 weeks. Viral most of the time. Bacterial in less than 5%. Patients with allergic rhinitis (AR) are more susceptible to acute sinusitis.
Duration of symptoms and definition
Less than 4 weeks - acute sinusitis
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
Nasal physiology
Mucociliary clearance can be tested by placing saccharin on the inferior turbinate and timing the onset of sweet taste in the mouth. The normal range is 7-11 minutes.
There is normal asymmetry of nasal mucosa swelling, with one side of nose swollen as a result of dilatation of veins in the inferior turbinate and the other side "open" - 80% of the population exhibits a nasal cycle, with reciprocal changes in airflow over 1-2 hours.
Anatomy
Sinus is a Latin word for “fold” or “pocket”. Paranasal sinuses have an embryogenic origin from the nasal passage and are an integral component of the airway. Drainage pathways of the sinuses are complex and can be blocked during inflammation. Ostia are the sinus openings in the nasal cavity. They are 2-6 mm wide.
Location of the openings of the sinuses
- Inferior meatus - opening of nasolacrimal duct.
- Middle meatus - frontal, maxillary and anterior ethmoids
- Superior turbinate - posterior ethmoids and sphenoid sinuses
Mnemonic
Sinuses listen to the following radio channels: FM AM / PS SS
Frontal sinus, Maxillary sinus, and
Anterior ethmoids drain into Middle meatus
Posterior ethmoids and Sphenoid sinus drain into
Sphenoethmoidal recess above Superior turbinate
Sinusitis
Approximately 31-35 million Americans are affected by sinusitis every year (15% of the population).
Sinusitis of less than 4 weeks’ duration is considered acute. Chronic sinusitis persists for more than 4 weeks.
Recurrent sinusitis is defined as 4 or more episodes of sinusitis per year. Each episode lasting 7-10 days and no symptoms during intervening periods.
Acute Exacerbation of Chronic Sinusitis is the sudden worsening of chronic sinusitis that returns to baseline with treatment.
The term sinusitis is often interpreted as reflecting simply a bacterial sinus infection but the disease can have a significant allergic component.
Sinusitis is mostly preceded by rhinitis and is rarely found without rhinitis.
The 1997 Rhinosinusitis Task Force thus proposed the term Rhinosinusitis instead of Sinusitis (reiterated in 2007 guidelines).
Acute Sinusitis
Symptoms for up to 4 weeks. Viral most of the time. Bacterial in less than 5%. Patients with allergic rhinitis (AR) are more susceptible to acute sinusitis.
Duration of symptoms and definition
Less than 4 weeks - acute sinusitis
4-12 weeks - subacute sinusitis
Longer than 12 weeks - chronic sinusitis
Complications of acute sinusitis
Orbital cellulitis
Subperiostal, intraorbital or eyelid abscess
Cavernous sinus thrombosis
Meningitis
Subdural, epidural or brain abscesses
Osteomyelitis of frontal bone (Potts puffy tumor)
Chronic Sinusitis
Symptoms for more than 12 weeks. Not an "infection."
Eosinophilic Sinusitis
Allergic Fungal Sinusitis (click to read the article)
Complications of acute sinusitis
Orbital cellulitis
Subperiostal, intraorbital or eyelid abscess
Cavernous sinus thrombosis
Meningitis
Subdural, epidural or brain abscesses
Osteomyelitis of frontal bone (Potts puffy tumor)
Chronic Sinusitis
Symptoms for more than 12 weeks. Not an "infection."
Eosinophilic Sinusitis
Allergic Fungal Sinusitis (click to read the article)
Noneosinophilic Sinusitis
Noneosinophilic sinusitis is considered to have an infectious basis and is treated with antibiotics. Organisms found are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. If a patient has Pseudomonas aeruginosa or Staphylococcus aureus, cystic fibrosis should be considered in differential diagnosis.
Diagnosis
A limited CT of sinuses costs about the same as a standard plain film sinus series but is much more useful.
CT scan findings do not correlate well with symptoms.
Upper airway endoscopy can identify anatomic or mechanical disorders of the upper airway. Anterior rhinoscopy is an examination of the nasal cavity performed with a nasal speculum under good illumination. Usually done with a rigid rhinoscope.
The gold standard for diagnosis of bacterial sinusitis is sinus puncture and culture.
Treatment
Treatment of Acute Sinusitis
Over 70% of patients with acute rhinosinusitis improve after 7 days, with or without antimicrobial therapy.
NNT = 7: 7 patients must be treated to achieve one additional positive outcome at 7 to 12 days.
More adverse effects in treated group, number needed to harm (NNH) = 9.
Start antibiotics if no improvement by day 7 or patient has worsening at any time.
Amoxicillin should be first choice based on safety, efficacy, cost, and narrow spectrum. A 10-14 day course is commonly used (7 days beyond clinical improvement).
Treatment of Chronic Sinusitis
Saline lavage (Ann Fam Medicine, July 2006).
Intranasal steroids (INS)
Antihistamines – not useful, may worsen by drying mucosa. Only consider if significant allergic component.
Itraconazole (Sporanox) for fungal sinusitis (most commonly seen in the Southern states). Itraconazole use requires a close follow-up due to the risk of CHF, cardiac arrhythmias, liver dysfunction and peripheral neuropathy (foot drop). It has a "black box" warning for CHF patients.
Refer to ENT for chronic sinusitis. Balloon sinuplasty is a procedure gaining wider acceptance.
Nasal Polyps
Nasal polyps can be considered a form of chronic hyperplastic sinusitis and usually originate in the ethmoid sinuses. Malignant transformation is uncommon. Polyps can occupy the entire nasal cavity, thus producing a total blockage.
Nasal polyposis can be associated with allergic fungal sinusitis, cystic fibrosis (CF) and the triad of asthma, aspirin intolerance, and nasal polyps (Samter's triad in AERD). In cystic fibrosis, polyps show neutrophilic inflammation.
CF should always be considered in children with nasal polyps.
What is the triad of aspirin-exacerbated respiratory disease (AERD)?
Samter's triad include asthma, aspirin sensitivity, and nasal/ethmoidal polyposis:
ASPirin
Asthma
Sensitivity to aspirin
Polyps
Approximately 9% of the U.S. population has asthma - 9% of adult asthmatics have aspirin-exacerbated respiratory disease (AERD) (http://goo.gl/FIeE9).
Noneosinophilic sinusitis is considered to have an infectious basis and is treated with antibiotics. Organisms found are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. If a patient has Pseudomonas aeruginosa or Staphylococcus aureus, cystic fibrosis should be considered in differential diagnosis.
Diagnosis
A limited CT of sinuses costs about the same as a standard plain film sinus series but is much more useful.
CT scan findings do not correlate well with symptoms.
Upper airway endoscopy can identify anatomic or mechanical disorders of the upper airway. Anterior rhinoscopy is an examination of the nasal cavity performed with a nasal speculum under good illumination. Usually done with a rigid rhinoscope.
The gold standard for diagnosis of bacterial sinusitis is sinus puncture and culture.
Treatment
Treatment of Acute Sinusitis
Over 70% of patients with acute rhinosinusitis improve after 7 days, with or without antimicrobial therapy.
NNT = 7: 7 patients must be treated to achieve one additional positive outcome at 7 to 12 days.
More adverse effects in treated group, number needed to harm (NNH) = 9.
Start antibiotics if no improvement by day 7 or patient has worsening at any time.
Amoxicillin should be first choice based on safety, efficacy, cost, and narrow spectrum. A 10-14 day course is commonly used (7 days beyond clinical improvement).
Treatment of Chronic Sinusitis
Saline lavage (Ann Fam Medicine, July 2006).
Intranasal steroids (INS)
Antihistamines – not useful, may worsen by drying mucosa. Only consider if significant allergic component.
Itraconazole (Sporanox) for fungal sinusitis (most commonly seen in the Southern states). Itraconazole use requires a close follow-up due to the risk of CHF, cardiac arrhythmias, liver dysfunction and peripheral neuropathy (foot drop). It has a "black box" warning for CHF patients.
Refer to ENT for chronic sinusitis. Balloon sinuplasty is a procedure gaining wider acceptance.
Nasal Polyps
Nasal polyps can be considered a form of chronic hyperplastic sinusitis and usually originate in the ethmoid sinuses. Malignant transformation is uncommon. Polyps can occupy the entire nasal cavity, thus producing a total blockage.
Nasal polyposis can be associated with allergic fungal sinusitis, cystic fibrosis (CF) and the triad of asthma, aspirin intolerance, and nasal polyps (Samter's triad in AERD). In cystic fibrosis, polyps show neutrophilic inflammation.
CF should always be considered in children with nasal polyps.
What is the triad of aspirin-exacerbated respiratory disease (AERD)?
Samter's triad include asthma, aspirin sensitivity, and nasal/ethmoidal polyposis:
ASPirin
Asthma
Sensitivity to aspirin
Polyps
Approximately 9% of the U.S. population has asthma - 9% of adult asthmatics have aspirin-exacerbated respiratory disease (AERD) (http://goo.gl/FIeE9).
Pediatric sinusitis (click the link to continue).
Surgical treatment of chronic sinusitis
References
Allergy and Immunology MKSAP, 3rd edition.
Acute and Chronic Rhinosinusitis: Practical Clinical Treatment Strategies. Nancy Otto, PharmD. Medscape, 11/2008.
Acute Sinusitis: A Cost-Effective Approach to Diagnosis and Treatment. AFP, 1998.
Sinusitis Practice Guideline Aims to Improve Diagnosis, Cut Antibiotic Use. AFP, 2007.
Related Reading
FIT Corner Questions. Chapter 78 of the 6th edition of Middleton’s Allergy Principles and Practice, edited by N. Franklin Adkinson, et al. September 27, 2006. Chapter 78: Nasal Polyps and Sinusitis.
Allergic Fungal Sinusitis. Photoclinic. Consultant. Vol. 48 No. 9, August 1, 2008.
JAMA Patient Page: Acute Sinusitis, 2009.
Surgical treatment of chronic sinusitis
Functional Endoscopic Sinus Surgery (FESS) is the surgical standard of care. FESS restores sinus drainage and provides some symptom improvement in close to 90% of selected patients.
References
Allergy and Immunology MKSAP, 3rd edition.
Pediatric sinusitis. Ellen R. Wald, MD. Audio-Digest Pediatrics, Volume 55, Issue 14, July 21, 2009.
Acute Bacterial Rhinosinusitis in Adults: Part II. Treatment. AFP, 2004.Acute and Chronic Rhinosinusitis: Practical Clinical Treatment Strategies. Nancy Otto, PharmD. Medscape, 11/2008.
Acute Sinusitis: A Cost-Effective Approach to Diagnosis and Treatment. AFP, 1998.
Sinusitis Practice Guideline Aims to Improve Diagnosis, Cut Antibiotic Use. AFP, 2007.
Related Reading
FIT Corner Questions. Chapter 78 of the 6th edition of Middleton’s Allergy Principles and Practice, edited by N. Franklin Adkinson, et al. September 27, 2006. Chapter 78: Nasal Polyps and Sinusitis.
Allergic Fungal Sinusitis. Photoclinic. Consultant. Vol. 48 No. 9, August 1, 2008.
JAMA Patient Page: Acute Sinusitis, 2009.
Humming increases airflow between the sinus and nasal cavities, which could protect against sinus infections. NYTimes, 2010.
Multi-symptom Asthma is Closely Related to Nasal Blockage, Rhinorrhea and Symptoms of Chronic Rhinosinusitis http://goo.gl/sU4AU
Nucleotide-binding oligomerization domain (NOD)-like receptors (NLRs) have a potential role in chronic rhinosinusitis/polyps http://goo.gl/QAS4r
Atrophic Rhinosinusitis: Progress Toward Explanation of an Unsolved Medical Mystery. Medscape, 2011.
SNOT-16 Assessment Tool for Acute Sinusitis takes 5 minutes - copyright protected by Washington University. Medscape, 2011.
Staphylococcus aureus biofilm and and superantigens are associated with chronic sinusitis, cause T-helper 2 skewing http://bit.ly/ngnxBe
Intranasal antinuclear autoantibodies (ANA) in patients with chronic rhinosinusitis with nasal polyps. JACI, 2011.
Chronic Sinusitis - JAMA Patient Page (PDF), 2011.
Mnemonics for sinusitis: PODS and C-PODS (end of PDF here)
Published: 07/10/2007
Updated: 04/29/2012
SNOT-16 Assessment Tool for Acute Sinusitis takes 5 minutes - copyright protected by Washington University. Medscape, 2011.
Staphylococcus aureus biofilm and and superantigens are associated with chronic sinusitis, cause T-helper 2 skewing http://bit.ly/ngnxBe
Intranasal antinuclear autoantibodies (ANA) in patients with chronic rhinosinusitis with nasal polyps. JACI, 2011.
Chronic Sinusitis - JAMA Patient Page (PDF), 2011.
Mnemonics for sinusitis: PODS and C-PODS (end of PDF here)
Published: 07/10/2007
Updated: 04/29/2012
How to treat rhinitis medicamentosa?
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 47-year-old Caucasian male was seen by the allergy clinic for allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa 4 weeks ago. He had been using Afrin several times a day for three years with gradual increase in nasal congestion and increasingly disturbed sleep and dry mouth. During the last visit, we stopped the Afrin and prescribed a prednisone taper starting at 40 mg po daily and continuing for 15 . He also had evidence of nasal polyposis on both sides and a right nasal polyp. We prescribed Singulair 10 mg po daily and Veramyst one spray in each nostril daily.
Approximately 20 days after the last visit, just after he finished his oral taper of steroids, he called back the clinic because of increased nasal congestion. We added a sinus rinse twice a day to his regimen and he felt a substantial relief. He rates his nasal symptoms as 5 out of 10, down from 8 out of 10 during the last visit (on a 0 to 10 scale). Currently, he is using a nasal spray in the evening and nasal rinse in the evening as well and reports feeling much better.
Past medical history (PMH)
Allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa. Nasal polyposis. HTN. He had skin-prick test during the last visit and it was moderately positive to trees, black willow, and marginally positive reaction to weeds, English plantain, and mild reaction to two of the molds.
Medications
Veramyst one spray daily, Singulair 10 mg po daily, Allegra 60 mg po b.i.d., Atacand 4 mg po daily.
Social history
Unremarkable.
Family history
Adopted.
Physical Examination
Vital signs: Stable.
Skin: No rashes.
Ears: Normal. Nose: Pale, boggy turbinates, mucoid discharge, polypoid changes on both sides and a nasal polyp on the right. Throat: Postnasal drip and cobblestoning.
Chest: clear to auscultation bilaterally. Cardiovascular system: Clear S1, S2. Abdomen: Soft, non-tender, non-distended. Extremities: No edema.
What is the most likely diagnosis?
Rhinitis medicamentosa and nasal polyposis.
What tests would you suggest?
Asthma often coincides with allergic rhinitis. A spirometry was done and it was normal.
What treatment would you suggest?
This is a patient with allergic rhinitis, non-allergic rhinitis, rhinitis medicamentosa, and nasal polyps. The combination of intranasal steroids and leukotriene antagonist is indicated, and we decided to continue the same treatment. He still has symptoms of nasal congestion, which is expected with the gradual resolution of his rhinitismedicamentosa. We recommended he should stay off Afrin. He should increase the dose of intranasal steroid to twice a day and also use the nasal rinses b.i.d. He is to follow up with us in three months.
Final diagnosis
Allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa. Nasal polyposis.

Afrin - Costco.
References
Rhinitis Medicamentosa. eMedicine Specialties > Allergy and Immunology > Medical Topics, 2006.
Diagnosing Rhinitis: Allergic vs. Nonallergic. AFP, 2006.
Vasomotor Rhinitis. AFP, 2005.
Nasal Sprays Can Bring on Vicious Cycle. NYTimes, 2006.
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 47-year-old Caucasian male was seen by the allergy clinic for allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa 4 weeks ago. He had been using Afrin several times a day for three years with gradual increase in nasal congestion and increasingly disturbed sleep and dry mouth. During the last visit, we stopped the Afrin and prescribed a prednisone taper starting at 40 mg po daily and continuing for 15 . He also had evidence of nasal polyposis on both sides and a right nasal polyp. We prescribed Singulair 10 mg po daily and Veramyst one spray in each nostril daily.
Approximately 20 days after the last visit, just after he finished his oral taper of steroids, he called back the clinic because of increased nasal congestion. We added a sinus rinse twice a day to his regimen and he felt a substantial relief. He rates his nasal symptoms as 5 out of 10, down from 8 out of 10 during the last visit (on a 0 to 10 scale). Currently, he is using a nasal spray in the evening and nasal rinse in the evening as well and reports feeling much better.
Past medical history (PMH)
Allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa. Nasal polyposis. HTN. He had skin-prick test during the last visit and it was moderately positive to trees, black willow, and marginally positive reaction to weeds, English plantain, and mild reaction to two of the molds.
Medications
Veramyst one spray daily, Singulair 10 mg po daily, Allegra 60 mg po b.i.d., Atacand 4 mg po daily.
Social history
Unremarkable.
Family history
Adopted.
Physical Examination
Vital signs: Stable.
Skin: No rashes.
Ears: Normal. Nose: Pale, boggy turbinates, mucoid discharge, polypoid changes on both sides and a nasal polyp on the right. Throat: Postnasal drip and cobblestoning.
Chest: clear to auscultation bilaterally. Cardiovascular system: Clear S1, S2. Abdomen: Soft, non-tender, non-distended. Extremities: No edema.
What is the most likely diagnosis?
Rhinitis medicamentosa and nasal polyposis.
What tests would you suggest?
Asthma often coincides with allergic rhinitis. A spirometry was done and it was normal.
What treatment would you suggest?
This is a patient with allergic rhinitis, non-allergic rhinitis, rhinitis medicamentosa, and nasal polyps. The combination of intranasal steroids and leukotriene antagonist is indicated, and we decided to continue the same treatment. He still has symptoms of nasal congestion, which is expected with the gradual resolution of his rhinitismedicamentosa. We recommended he should stay off Afrin. He should increase the dose of intranasal steroid to twice a day and also use the nasal rinses b.i.d. He is to follow up with us in three months.
Final diagnosis
Allergic rhinitis, non-allergic rhinitis, and rhinitis medicamentosa. Nasal polyposis.
Afrin - Costco.
References
Rhinitis Medicamentosa. eMedicine Specialties > Allergy and Immunology > Medical Topics, 2006.
Diagnosing Rhinitis: Allergic vs. Nonallergic. AFP, 2006.
Vasomotor Rhinitis. AFP, 2005.
Nasal Sprays Can Bring on Vicious Cycle. NYTimes, 2006.
Pseudoephedrine used in allergic rhinitis improved stuffy nose but decreased sexual activity http://goo.gl/1uLxb
Oxymetazoline for 1 month adds to nasal steroid effect in perennial allergic rhinitis, without development of rhinitis medicamentosa. JACI, 2011.
Published: 03/03/2009
Updated: 02/03/2011
Published: 03/03/2009
Updated: 02/03/2011
Allergic Rhinitis and Conjunctivitis
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 35-year-old CF is referred to the allergy clinic for symptoms of allergic rhinitis and conjunctivitis. She complains of itchy and watery eyes, itchy nose, nasal congestion, postnasal drip, itching in her ear and throat. These symptoms are seasonal and occur predominantly during the spring and summer. Triggers include exposure to grass. She has tried over-the-counter medications with good relief of symptoms but it does not last long enough. Immunotherapy has never been tried. No history of nasal polyps, eczema, food allergies, or systemic reactions to stinging insects.
Past medical history (PMH)
Exercise-induced asthma. She was on Azmacort and SABA (albuterol) PRN. A recent PFT and methacholine challenge test were reported as normal, and she was instructed to stop Azmacort and use albuterol prn for SOB on exertion.
Hives. She has intermittent episodes of single lesions that occur mostly over the arms and occasionally on the face. The lesions would disappear spontaneously within 24 hours. There are no identifiable triggers, specifically the hives are not related to ASA, NSAIDs or other medications, physical or temperate triggers. Episodes are mild that she does not feel an evaluation or medical therapy is needed.
Medications
Fluticasone (Flonase) 50 mcg/actuation nasal spray QHS, albuterol 90 PRN
SH
No tobacco or alcohol use
Environmental history
Pets in the home: 2 dogs. Flooring: Wall-to-wall carpeting. Air conditioning: Central air. Heating: Forced hot air. Basement: Dry basement. Dust mite controls: Dust mite controls are not in place. Tobacco smoke: no exposure in the home.
FH
Mother with asthma
Physical examination
VSS
HEENT: External ears normal. Canals clear. TM's normal. Nares normal. Septum midline. Congested pale mucosa, no polyps seen. No drainage or sinus tenderness. Lips, tongue normal. Oropharynx clear.
Neck: supple, no adenopathy
CVS: RRR, normal S1/S2, no m/r/g
Chest: CTA (B)
Extremities: no c/c/e
Skin: color, texture, turgor normal. No rashes or lesions.
What is the most likely diagnosis?
Allergic rhinitis and conjunctivitis.
What tests would you order?
Skin prick testing.
What happened?
The allergen skin testing was positive as below:
Mold 2+
Trees 3+
Grass 4+
Weeds 2+
Ragweed 3+
What happened next?
The patient has allergic rhinitis with throat, eyes, and nasal symptoms during spring and summer seasons. She also has positive skin testing to grass, weeds, trees and mold.
Flonase was continued at a dose of 50 mcg nasal spray 1 squirt daily, she was advised to avoid septum when spraying. She was also instructed to increase Flonase to 2 squirts daily if symptoms worsen. Olopatadine (Patanol) 2 drops in both eyes bid was prescribed for control of her ocular symptoms. If symptoms are still not under control, she was advised to call the office for possibly adding an oral antihistamine.
Medication dosage, usage, side effects and goal of treatment were discussed. She was advised on the benefits of being indoors with air conditioning during spring, summer and fall.
Risks and benefits of immunotherapy for allergic rhinitis were discussed and the patient opted to start immunotherapy. A follow-up in 1 month was arranged.
Final diagnosis
Allergic rhinitis and conjunctivitis.
What did we learn from this case?
What nasal spray provides relief in 30 minutes in allergic rhinitis?
Patanase (olopatadine) is currently the only nasal spray to provide relief in 30 minutes in allergic rhinitis. The effect lasts for 12 hours.

Allergic rhinitis mind map.

Medications for Allergic Rhinitis
Treatment Options for Allergic Rhinitis (click to enlarge the image).

Ocular antihistamines (eye drops) (click to enlarge the image).
References
Rhinitis, Allergic. eMedicine, 2007.
Allergic Rhinitis. eMedicine, 2007.
Seasonal Allergic Rhinitis: A Short Review. V. Dimov, M.D., 2007.
FDA Approvals: Patanase, Actonel, Cimzia. Medscape, 2008.
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
A 35-year-old CF is referred to the allergy clinic for symptoms of allergic rhinitis and conjunctivitis. She complains of itchy and watery eyes, itchy nose, nasal congestion, postnasal drip, itching in her ear and throat. These symptoms are seasonal and occur predominantly during the spring and summer. Triggers include exposure to grass. She has tried over-the-counter medications with good relief of symptoms but it does not last long enough. Immunotherapy has never been tried. No history of nasal polyps, eczema, food allergies, or systemic reactions to stinging insects.
Past medical history (PMH)
Exercise-induced asthma. She was on Azmacort and SABA (albuterol) PRN. A recent PFT and methacholine challenge test were reported as normal, and she was instructed to stop Azmacort and use albuterol prn for SOB on exertion.
Hives. She has intermittent episodes of single lesions that occur mostly over the arms and occasionally on the face. The lesions would disappear spontaneously within 24 hours. There are no identifiable triggers, specifically the hives are not related to ASA, NSAIDs or other medications, physical or temperate triggers. Episodes are mild that she does not feel an evaluation or medical therapy is needed.
Medications
Fluticasone (Flonase) 50 mcg/actuation nasal spray QHS, albuterol 90 PRN
SH
No tobacco or alcohol use
Environmental history
Pets in the home: 2 dogs. Flooring: Wall-to-wall carpeting. Air conditioning: Central air. Heating: Forced hot air. Basement: Dry basement. Dust mite controls: Dust mite controls are not in place. Tobacco smoke: no exposure in the home.
FH
Mother with asthma
Physical examination
VSS
HEENT: External ears normal. Canals clear. TM's normal. Nares normal. Septum midline. Congested pale mucosa, no polyps seen. No drainage or sinus tenderness. Lips, tongue normal. Oropharynx clear.
Neck: supple, no adenopathy
CVS: RRR, normal S1/S2, no m/r/g
Chest: CTA (B)
Extremities: no c/c/e
Skin: color, texture, turgor normal. No rashes or lesions.
What is the most likely diagnosis?
Allergic rhinitis and conjunctivitis.
What tests would you order?
Skin prick testing.
What happened?
The allergen skin testing was positive as below:
Mold 2+
Trees 3+
Grass 4+
Weeds 2+
Ragweed 3+
What happened next?
The patient has allergic rhinitis with throat, eyes, and nasal symptoms during spring and summer seasons. She also has positive skin testing to grass, weeds, trees and mold.
Flonase was continued at a dose of 50 mcg nasal spray 1 squirt daily, she was advised to avoid septum when spraying. She was also instructed to increase Flonase to 2 squirts daily if symptoms worsen. Olopatadine (Patanol) 2 drops in both eyes bid was prescribed for control of her ocular symptoms. If symptoms are still not under control, she was advised to call the office for possibly adding an oral antihistamine.
Medication dosage, usage, side effects and goal of treatment were discussed. She was advised on the benefits of being indoors with air conditioning during spring, summer and fall.
Risks and benefits of immunotherapy for allergic rhinitis were discussed and the patient opted to start immunotherapy. A follow-up in 1 month was arranged.
Final diagnosis
Allergic rhinitis and conjunctivitis.
What did we learn from this case?
What nasal spray provides relief in 30 minutes in allergic rhinitis?
Patanase (olopatadine) is currently the only nasal spray to provide relief in 30 minutes in allergic rhinitis. The effect lasts for 12 hours.

Allergic rhinitis mind map.

Medications for Allergic Rhinitis
Treatment Options for Allergic Rhinitis (click to enlarge the image).
Ocular antihistamines (eye drops) (click to enlarge the image).
References
Rhinitis, Allergic. eMedicine, 2007.
Allergic Rhinitis. eMedicine, 2007.
Seasonal Allergic Rhinitis: A Short Review. V. Dimov, M.D., 2007.
FDA Approvals: Patanase, Actonel, Cimzia. Medscape, 2008.
Fluticasone furoate nasal spray is the only intranasal corticosteroid to reduce the ocular symptoms of seasonal allergic rhinitis consistently, JACI, 2010. http://goo.gl/oQ2n2
Published: 09/14/2007
Updated: 02/24/2011
Published: 09/14/2007
Updated: 02/24/2011
More than a "runny nose" - allergic rhinitis and asthma
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
An 11-year-old Caucasian boy is referred by his primary care physician mother for nasal congestion and runny nose for years. His symptoms are not getting worse, but they are persistent. He was on fluticasone (Flonase) in the past off and on with history of noncompliance and he did not feel that Flonase helped significantly. Approximately two months ago, he started to complain of shortness of breath, dyspnea on exertion and cough. The symptoms start approximately 15 to 20 minutes after he starts exercising, and they resolve after he stops exercising. He has no night symptoms. He has symptoms throughout the year with worse nasal congestion in August and September.
Past medical history (PMH)
Allergic rhinitis.
Medications
Montelukast (Singulair) 5 mg po daily.
Social history
He is not exposed to tobacco. Pets: He has a hamster and a dog. The dog is a golden retriever.
Family history
Mother and father with allergic rhinitis, siblings with allergic rhinitis and atopic eczema.
Physical examination
Thin boy in no apparent distress.
Vital signs stable. Temperature 98.8 F, heart rate 80 bpm, respiratory rate 18, blood pressure 110/60 mm/Hg.
Skin: No rashes.
Eyes: Normal. Ears: Normal.
Nose: Pale, boggy turbinates. Throat: Normal.
Respiratory system: Clear to auscultation bilaterally, no wheezing, rhonchi or crackles. Cardiovascular system: Clear S1, S2.
Abdomen: Soft, non-tender, non-distended. Extremities: No cyanosis, clubbing, or edema.
What is the most likely diagnosis?
- Allergic rhinitis
- Asthma
What tests would you suggest?
- Skin prick testing
- Spirometry
Skin prick testing was done with a positive reaction to histamine. All other allergens in the pediatric allergy panel were negative.
The baseline spirometry revealed a FVC of 80% and a FEV1 of 75%.
What tests would you suggest next?
We a performed bronchodilator test with 4 puffs of albuterol and the patient’s values improved greatly. His FEV1 improved by 24% from 1.45 liters to 1.81 liters, which satisfied the criteria for positive bronchodilator test for asthma. His FVC improved by 14% and his FEF-25-75% volumes improved by 56%.
What happened?
This is a patient with asthma with symptoms of exercise-induced bronchospasm and the diagnosis was confirmed by a 24% improvement in FEV1 on the bronchodilator test. We prescribed fluticasone (Flovent Diskus) 100 mcg, one inhalation b.i.d. He has also symptoms of allergic/ non-allergic rhinitis and for that, we prescribed budesonide (Rhinocort) nasal spray one spray in each nostril daily. He is to follow up with us in two months.
Final diagnosis
Asthma with symptoms of exercise-induced bronchospasm. Allergic and non-allergic rhinitis.
Summary
Asthma is the most common chronic respiratory disease, affecting up to 10% of adults and 30% of children (JACI, 2011).
Most patients with asthma have rhinitis suggesting the concept of ‘one airway one disease’ or ‘united airways’.
Prevalence of asthma in:
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at NSU
An 11-year-old Caucasian boy is referred by his primary care physician mother for nasal congestion and runny nose for years. His symptoms are not getting worse, but they are persistent. He was on fluticasone (Flonase) in the past off and on with history of noncompliance and he did not feel that Flonase helped significantly. Approximately two months ago, he started to complain of shortness of breath, dyspnea on exertion and cough. The symptoms start approximately 15 to 20 minutes after he starts exercising, and they resolve after he stops exercising. He has no night symptoms. He has symptoms throughout the year with worse nasal congestion in August and September.
Past medical history (PMH)
Allergic rhinitis.
Medications
Montelukast (Singulair) 5 mg po daily.
Social history
He is not exposed to tobacco. Pets: He has a hamster and a dog. The dog is a golden retriever.
Family history
Mother and father with allergic rhinitis, siblings with allergic rhinitis and atopic eczema.
Physical examination
Thin boy in no apparent distress.
Vital signs stable. Temperature 98.8 F, heart rate 80 bpm, respiratory rate 18, blood pressure 110/60 mm/Hg.
Skin: No rashes.
Eyes: Normal. Ears: Normal.
Nose: Pale, boggy turbinates. Throat: Normal.
Respiratory system: Clear to auscultation bilaterally, no wheezing, rhonchi or crackles. Cardiovascular system: Clear S1, S2.
Abdomen: Soft, non-tender, non-distended. Extremities: No cyanosis, clubbing, or edema.
What is the most likely diagnosis?
- Allergic rhinitis
- Asthma
What tests would you suggest?
- Skin prick testing
- Spirometry
Skin prick testing was done with a positive reaction to histamine. All other allergens in the pediatric allergy panel were negative.
The baseline spirometry revealed a FVC of 80% and a FEV1 of 75%.
What tests would you suggest next?
We a performed bronchodilator test with 4 puffs of albuterol and the patient’s values improved greatly. His FEV1 improved by 24% from 1.45 liters to 1.81 liters, which satisfied the criteria for positive bronchodilator test for asthma. His FVC improved by 14% and his FEF-25-75% volumes improved by 56%.
What happened?
This is a patient with asthma with symptoms of exercise-induced bronchospasm and the diagnosis was confirmed by a 24% improvement in FEV1 on the bronchodilator test. We prescribed fluticasone (Flovent Diskus) 100 mcg, one inhalation b.i.d. He has also symptoms of allergic/ non-allergic rhinitis and for that, we prescribed budesonide (Rhinocort) nasal spray one spray in each nostril daily. He is to follow up with us in two months.
Final diagnosis
Asthma with symptoms of exercise-induced bronchospasm. Allergic and non-allergic rhinitis.
Summary
Asthma is the most common chronic respiratory disease, affecting up to 10% of adults and 30% of children (JACI, 2011).
Most patients with asthma have rhinitis suggesting the concept of ‘one airway one disease’ or ‘united airways’.
Prevalence of asthma in:
- patients without rhinitis - less than 2%
- patients with rhinitis - 10-40%
Most patients with allergic or nonallergic asthma present with rhinitis symptoms. However, not all patients with rhinitis present with asthma.
Many patients with allergic rhinitis have an increased bronchial reactivity to methacholine.
Childhood allergic rhinitis is associated with a 2- to 7-fold increased risk of asthma in preadolescence, adolescence, or adult life.
On average, childhood allergic rhinitis was associated with a 3-fold increased risk of childhood asthma persisting compared with remitting by middle age. Asthma burden in later life might be reduced by more aggressive treatment of allergic rhinitis in early life.
It is not clear if treatment of one airway will improve symptoms of the other site.
The 1999 WHO workshop ‘Allergic Rhinitis and its Impact on Asthma’ recommended:
- patients with persistent allergic rhinitis should be evaluated for asthma by history, chest examination, and possibly assessment of airflow obstruction before and after bronchodilator
- history and examination of the upper respiratory tract for allergic rhinitis should be performed in patients with asthma
Treatment Options for Allergic Rhinitis (click to enlarge the image).
References
Childhood allergic rhinitis predicts asthma incidence and persistence to middle age: A longitudinal study. J Allergy Clin Immunol. 2007 Sep 6.
Links between allergic rhinitis and asthma still reinforced. P. Demoly, P. J. Bousquet (2008). Allergy 63 (3), 251–254.
Serum eosinophil granule proteins predict asthma risk in allergic rhinitis. Nielsen LP, Peterson CG, Dahl R. Allergy. 2008 Dec 24.
Related reading
How to predict risk of developing asthma in allergic rhinitis? Use serum eosinophil granule proteins ECP and EPO
- patients with rhinitis - 10-40%
Most patients with allergic or nonallergic asthma present with rhinitis symptoms. However, not all patients with rhinitis present with asthma.
Many patients with allergic rhinitis have an increased bronchial reactivity to methacholine.
Childhood allergic rhinitis is associated with a 2- to 7-fold increased risk of asthma in preadolescence, adolescence, or adult life.
On average, childhood allergic rhinitis was associated with a 3-fold increased risk of childhood asthma persisting compared with remitting by middle age. Asthma burden in later life might be reduced by more aggressive treatment of allergic rhinitis in early life.
It is not clear if treatment of one airway will improve symptoms of the other site.
The 1999 WHO workshop ‘Allergic Rhinitis and its Impact on Asthma’ recommended:
- patients with persistent allergic rhinitis should be evaluated for asthma by history, chest examination, and possibly assessment of airflow obstruction before and after bronchodilator
- history and examination of the upper respiratory tract for allergic rhinitis should be performed in patients with asthma
Treatment Options for Allergic Rhinitis (click to enlarge the image).
References
Childhood allergic rhinitis predicts asthma incidence and persistence to middle age: A longitudinal study. J Allergy Clin Immunol. 2007 Sep 6.
Links between allergic rhinitis and asthma still reinforced. P. Demoly, P. J. Bousquet (2008). Allergy 63 (3), 251–254.
Serum eosinophil granule proteins predict asthma risk in allergic rhinitis. Nielsen LP, Peterson CG, Dahl R. Allergy. 2008 Dec 24.
Related reading
How to predict risk of developing asthma in allergic rhinitis? Use serum eosinophil granule proteins ECP and EPO
Forced expiratory flow between 25-75% of vital capacity may be a marker of bronchial impairment in allergic rhinitis http://goo.gl/yTNW2
Rhinitis is common in asthma and impairs asthma control. Allergy. 2011.
What symptom works best for diagnosis of allergic rhinitis? The answer has been the same for years: eye itching (http://goo.gl/koioJ).
Poor asthma control? – then look up the nose. The importance of co-morbid rhinitis in patients with asthma http://goo.gl/0nNZg
Published: 02/11/2009
Updated: 05/11/2012
Rhinitis is common in asthma and impairs asthma control. Allergy. 2011.
What symptom works best for diagnosis of allergic rhinitis? The answer has been the same for years: eye itching (http://goo.gl/koioJ).
Poor asthma control? – then look up the nose. The importance of co-morbid rhinitis in patients with asthma http://goo.gl/0nNZg
Published: 02/11/2009
Updated: 05/11/2012
Mind Maps: Allergic Rhinitis
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
Treatment Options for Allergic Rhinitis (AR) and Non-Allergic Rhinitis (NAR) (click to enlarge the image).

Allergic (atopic) march (click here to enlarge the image).
Allergic rhinitis mind map.
Medications for Allergic Rhinitis.

Rhinitis types, pathological classification (click to enlarge the image).
Treatment Options for Allergic Rhinitis (click to enlarge the image).
Published: 01/24/2008
Updated: 12/21/2012
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology
Treatment Options for Allergic Rhinitis (AR) and Non-Allergic Rhinitis (NAR) (click to enlarge the image).
Allergic (atopic) march (click here to enlarge the image).
Allergic rhinitis mind map.
Medications for Allergic Rhinitis.

Rhinitis types, pathological classification (click to enlarge the image).
Treatment Options for Allergic Rhinitis (click to enlarge the image).
Published: 01/24/2008
Updated: 12/21/2012
Ocular Allergy: Allergic Conjunctivitis and Related Conditions, Brief Review
Author: V. Dimov, M.D., Allergist/Immunologist and Assistant Professor at University of Chicago
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology

Classification of ocular allergy (click to enlarge the image).

Alphabet "soup": SAC, PAC, AKC, VKC, GPC (click to enlarge the image).
Allergic Conjunctivitis
- AAC
- SAC
- PAC
Keratoconjunctivitis
- Atopic Keratoconjunctivitis (AKC), atopic dermatitis-related, lower eyelid
- Vernal Keratoconjunctivitis (VKC), upper eyelid. See Vernal Keratoconjunctivitis - NEJM images, 2012.
Giant Papillary Conjunctivitis (GPC), contact lenses-related, upper eyelid
Contact dermatoconjunctivitis
All ocular allergies are characterized by bilateral involvement. Sensitization is necessary for all ocular allergies except for giant papillary conjunctivitis.
Most common type of ocular allergy is allergic conjunctivitis (80-90% of all cases).
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
Allergic conjunctivitis
Allergic conjunctivitis is a relatively benign disease that does not threaten vision. Ocular allergy is estimated to affect 20-25% of the population and the incidence is increasing.
Clinical Manifestations
Allergic conjunctivitis is a disease of young adults (average age of onset 20 years).
As with many allergic diseases, symptoms decrease with age.
50% of patients have a personal or family history of other allergic conditions such as allergic rhinitis, atopic dermatitis, and asthma
Signs and symptoms
Itching, tearing, conjunctival edema, hyperemia, watery discharge, burning, and photophobia, eyelid edema.
Laboratory findings
Allergic conjunctivitis is a clinical diagnosis.

Diagnostic Tests in Allergic Conjunctivitis (of academic interest) (click to enlarge the image).
Some tests of academic interest:
- Conjunctival scrapings show eosinophils in 80%
- Tear film and serum IgE levels are elevated
- Tear film mast cell activity is increased - measured by immunoassay for tryptase (unique to mast cells).
But rubbing by itself can result in a significant increase of tryptase in tears.
Conjunctival provocation test (CPT)
CPT is used to study AC and drug efficacies. Before undergoing a CPT, patients must first be skin tested to determine the appropriate allergen for each patient. The allergen extract is applied bilaterally into the conjunctival sac of the eyes.
At baseline, 2 visits (7 days apart) are used to establish the threshold dose of allergen (visit 1) and reproducibility (visit 2).
CPT is a double-blind, randomized test in which the test drug is applied to one eye and placebo to the other.
Types of allergic conjunctivitis
3 categories
- Acute allergic conjunctivitis (AAC)
- Seasonal allergic conjunctivitis (SAC)
- Perennial allergic conjunctivitis (PAC), less common and less severe than SAC
The main difference between SAC and PAC is the timing of the symptoms. SAC symptoms last a specific season. PAC symptoms last throughout the year.
Acute allergic conjunctivitis (AAC)
Sudden-onset hypersensitivity reaction caused by environmental exposure, for example, such as cat dander.
AAC can be severe and debilitating. However, most cases of AAC are self-limited to 24 hours and do not require long-term treatment.
Seasonal allergic conjunctivitis (SAC)
There are several synonyms for SAC: allergic conjunctivitis, hay-fever conjunctivitis, or allergic rhinoconjunctivitis.
SAC is a milder form of ocular allergy than AAC, typically associated with allergic rhinitis (AR).
SAC is most commonly triggered by ragweed or grass pollens.
SAC has a chronic course that corresponds to pollen seasons: tree pollens in the spring, grass pollens in the summer, and weed pollens in the late summer and fall.
Perennial allergic conjunctivitis (PAC)
PAC is a mild chronic allergic conjunctivitis related to year-round indoor allergens, for example, house dust mite (HDM), animal dander, and molds.
PAC is less common and less severe than SAC.
Pathophysiology
All 3 types result from type I IgE–mediated hypersensitivity, same as other atopic diseases.
Conjunctival scrapings show 2 phases (early and late) of the allergic response, same as other atopic diseases affecting the skin, nose and lungs.
The immediate response to allergens is mediated by mast cells, which are normally present in high concentrations in the conjunctiva.
Allergen-IgE crosslinking causes mast cells to release chemical mediators.
Histamine is the mediator of the early response.
Late response consists of cell influx (eosinophils, basophils, and neutrophils) which usually takes 6-10 hours after allergen challenge.
Eosinophils release leukotriene C4, eosinophilic peroxidase, eosinophilic cationic protein, and histamine into the tear fluid.
Diagnosis
The diagnosis of allergic conjunctivitis is usually clinically apparent in the context of typical history and physical examination findings.
The dominant symptom in AC is itching. The eye appears red. Typically, itch is not reported with dry eye.
Laboratory tests are not usually needed to confirm the clinical diagnosis of AC.
Differential diagnosis
- infectious conjunctivitis
- blepharitis
- dry eye
Allergic conditions are often accompanied by pruritus which is not common in infections.
Management
General measures:
- do not to rub the eyes. Eye rubbing causes mechanical mast cell degranulation.
- artificial tears several times a day
- allergen avoidance
- topical antihistamine eye drops
- cool compresses
-avoidance of contact lenses use -- allergens adhere to contact lens surfaces
Dry eyes or tear film insufficiency are extremely common.
Signs of tear film insufficiency include superficial punctate-keratopathy, reduced tear break-up time, and decreased production of tears as measured by the Schirmer's test.
Oral antihistamines can exacerbate tear film insufficiency through decreased tear production (anticholinergic effect).
Punctal plugs may be helpful and can be placed quickly and painlessly by an ophthalmologist.
Allergen avoidance
SAC:
- limit outdoor exposure
- air conditioning
- car and home windows closed
PAC:
- replacement of old pillows and mattresses
- covers for pillows and mattresses
- frequent washing of beddings
- reducing humidity
- frequent vacuuming and dusting of the home
- remove reservoirs of dust: old carpets, old furniture, old curtains or drapes
- if allergic to animal dander, remove the animal from the home
Immunotherapy
Immunotherapy is effective for treatment of allergic rhinoconjunctivitis
One meta-analysis included 15 studies of immunotherapy in patients with ocular allergy symptoms - 12 studies showed benefit -- decreased ocular symptoms scores and medication use.
Immunotherapy is useful treating ocular symptoms that coexist with allergic rhinitis or asthma but the its role in treating isolated ocular allergy is less clear.
Medications

Medications for Allergic Conjunctivitis (click to enlarge the image).
Medications for AAC
Most cases of AAC are self-limited to 24 hours and do not require long-term treatment.
Over-the-counter topical antihistamine/vasoconstrictor
Over-the-counter topical antihistamine/vasoconstrictor can be used to treat symptoms of short-duration (less than 2 weeks):
- Naphazoline/pheniramine maleate (Naphcon-A®, Opcon-A®, Visine-A®)
- Naphazoline/pheniramine phosphate (Vasocon-A®)
Topical vasoconstrictor (decongestants) work within minutes with a duration of 2 hours. Dosing is QID.
Use for longer than 2 weeks can lead to rebound hyperemia.
Antihistamines
Topical antihistamines are faster-acting than oral anthistimines and have little systemic effects.
The combination of a topical antihistamine and a vasoconstrictor works better than either agent alone.
Frequent attacks of AAC (more than 2 days per month) are treated with a dual-action agent (antihistamine/mast cell stabilizer) such as olopatadine.
Pataday® is used qd, Patanol® is used bid for prevention and qid for acute symptoms.
Other topical antihistamines and/or mast cell stabilizers: azelastine (Optivar®), epinastine (Elestat®), pemirolast (Alamast®), and ketotifen (generic).
Ketotifen bid is generic and over-the-counter.
Dual-acting, Antihistamine and Mast Cell–Stabilizing Drugs
These most commonly prescribed eye drops for allergic eye disease: azelastine, olopatadine, and ketotifen.
Medications for SAC and PAC
5 classes of topical drugs:
1. antihistamines
2. mast cell stabilizers, e.g. cromolyn
3. antihistamine/mast cell stabilizer combinations, e.g. olopatadine, ketotifen
4. steroids
5. non-steroidal anti-inflammatory agents (NSAIDs), e.g. ketorolac
Mnemonic for medications for SAC and PAC: MD VANS
Mast cell stabilizers
Dual-acting: antihistamine/mast cell stabilizer
Vasoconstrictors, not recommended
Antihistamines
NSAIDs, only ketorolac, not recommended
Steroids, only loteprednol, by opthalmologist
The treatment of choice for AC is dual–acting eye drops (antihistamine/mast cell stabilizer).
Treatment for SAC should be started 2 weeks prior to the onset of season which cases symptoms: tree pollens in the spring, grass pollens in the summer, and weed pollens in the late summer and fall.
Dual-action agents (topical antihistamines with mast cell stabilizing properties):
- olapatadine (Patanol®, Pataday®)
- azelastine HCl (Optivar®)
- epinastine (Elestat®)
- pemirolast (Alamast®)
- ketotifen (generic)
Ocular antihistamines (eye drops) (click to enlarge the image).
Mast cell stabilizers:
- cromolyn (generic, Opticrom®)
- lodoxamide (Alomide®)
The onset of action of mast cell stabilizers is slow (5-14 days) and the dosing is QID (inconvenient). Cromolyn cannot be used for acute symptoms.
One study compared cromolyn (4%, 4 times daily) for 2 weeks prior to allergen challenge to a single drop of ketotifen (0.025 percent) used just before the allergen challenge. The single drop of ketotifen was more effective.
Oral antihistamines
Oral antihistamines are less effective than topical olopatadine or topical ketotifen.
All antihistamines dry the ocular surface due to their atropine-like effect which decreases tear production of the lacrimal glands.
Oral antihistamines reach a peak serum levels in 0.5-3 hours depending on the drug but a full effects is after several days of use (similar to cromolyn). Oral antihistamines act much slower than topical antihistamines.
Cetirizine may cause sedation in a subset of patients, despite its categorization as non-sedating.
Topical NSAIDs
In theory, NSAIDs block the cyclooxygenase and inhibit the conversion of arachidonic acid to prostaglandins and thromboxanes.
In practice, NSAIDs are less effective than antihistanmines but more effective than placebo. NSAIDs are not recommended for treatment of allergic conjunctivitis.
Ketorolac is the only topical NSAID approved for itching due to AC.
Patients with AR and AC
Olopatadine can be combined with an intranasal steroid (INS). Fluticasone furoate nasal spray is the only intranasal corticosteroid to reduce the ocular symptoms of seasonal allergic rhinitis consistently, JACI, 2010.
When to refer to an ophthalmologist?
- Giant papillae occur on the upper tarsal plate and are described as cobblestoning.
- yellow-white points in the limbus (Trantas dots)
- yellow-white points on the conjunctiva (Horner points)
- corneal “shield” ulcers
- Dennie lines (Dennie-Morgan folds)
Shield ulcers are sterile ulcers which occur where cobblestone papillae are rubbing on cornea.
Children with VKC have measurably longer eyelashes (reaction to ocular inflammation).
VKC is chronic and sight-threatening.
Treatment of Vernal Keratoconjunctivitis
VKC is a sight-threatening disease.
Topical steroids 8 times per day for 7-10 days usually relieves symptoms.
High-dose aspirin therapy has been shown effective (2.4 gm daily)
Topical cyclosporin A (Restasis) has also been used in VKC: Cyclosporine eye drops prevent seasonal recurrences of vernal keratoconjunctivitis in a 2-year study (JACI, 2011).
Giant Papillary Conjunctivitis (GPC)
GPC is linked to chronic exposure to foreign bodies, such as contact lenses. GPC is considered an iatrogenic form of allergic eye disease.
Sensitization not necessary in GCP but is required in all other forms of ocular allergy.
GPC is a chronic inflammation that produces giant papillae (1 mm or greater) on the tarsal conjunctiva of the upper eyelids.
Causes of GPC:
- mechanical trauma secondary to contact lenses
- buildup of protein on the surface of the contact lens causes an allergic reaction
Treatment of Giant Papillary Conjunctivitis
Reduction in the wearing time of contact lenses or total discontinuation is required.
“Artificial tears” help to wash away environmental allergens and lens debris ("protein deposits").
Topical mast cell stabilizers are effective in the treatment of GPC and dual-acting drugs may be the best therapy.
Topical steroids are very effective but should be used only for a short period of time, e.g. 4 times per day for 2-4 days.
Contact lens can be resumed but it often requires a change in the type or material of the contact lenses.
Contact dermatoconjunctivitis
Contact dermatoconjunctivitis is a delayed cell-mediated hypersensitivity reaction (type IV), not an IgE antibody–mediated process.
Contact dermatitis involves the eyelids but can also involve the conjunctivae. Contact dermatitis may be caused by contact lens solutions but a multitude of irritants and allergens have been implicated, for example:
- eye drops, anesthetics, antiviral agents, pilocarpine, timolol
- preservatives in ophthalmic solutions (thiomersal, benzalkonium chloride, chlorhexidine, EDTA)
- cosmetics (eye glosses)
- perfumes
- sunscreens
- adhesives (false eyelashes)
Patch testing is the most useful diagnostic tool for contact dermatoconjunctivitis.
The best treatment is avoidance of the offending agent.
Immunologic Diseases of the Eye
Ocular cicatricial pemphigoid
Peripheral ulcerative keratitis
Episcleritis
Scleritis
Uveitis
List of optometric abbrevations
OU, oculus utro (each eye)
OS, oculus sinister (left eye)
OD, oculus dexter (right eye)
SPK, Superficial punctate keratitis
References
Allergic conjunctivitis. M Reza Dana, MD, MPH, MSc, UpToDate, 16.2, 8/2008.
Chapter 88 – Allergic and Immunologic Diseases of the Eye. Neal P. Barney, Frank M. Graziano. Adkinson: Middleton's Allergy: Principles and Practice, 6th ed.
Allergic Conjunctivitis. Presentation Materials. World Allergy Organization.
Pediatric Ocular Inflammation. Immunology and Allergy Clinic of North America. Volume 28, Issue 1, Pages 169-188 (February 2008).
Chapter 146 – Ocular Allergies. Mark Boguniewicz Donald Y.M. Leung. Kliegman: Nelson Textbook of Pediatrics, 18th ed.
Ocular Allergies. Ask the Expert. AAAAI.
Allergic Conjunctivitis. Ask the Expert. AAAAI.
Allergic conjunctivitis. Handbook of Ocular Disease Management.
Ocular Allergy. Curr Opin Allergy Clin Immunol. 2007; 7(5):424-428. Medscape. Medscape
The Pathophysiology of Ocular Allergy: Current Thinking. C Stephen Foster. Allergy, Volume 50 Issue s21, Pages 6 - 9, 2007.
Online Continuing Education: Ocular Allergy. University of Indiana.
Conjunctivitis, Allergic. Parag A Majmudar, MD. eMedicine.
Allergic rhinoconjunctivitis and differential diagnosis of the red eye. Granet, David. Allergy and Asthma Proceedings, Volume 29, Number 6, 11/12 2008 , pp. 565-574(10).
PowerPoint Presentations
Ocular allergy. V. Dimov, M.D., 09/2008.
Allergic Conjunctivitis. World Allergy Congress.
Allergic Conjunctivitis. MCFP.
Eye diseases and the internist. ACP.
Questions
Review Questions: Pediatric Allergy: Principles & Practices, Chapter 56: Allergic and Immunologic Eye Disease.
Patient information
Patient information: Eye Allergies. WebMD.
Ocular Allergies. Clifford W. Bassett, MD, FAAAAI. Allergy & Asthma Advocate: Summer 2007.
Reviewer: S. Randhawa, M.D., Allergist/Immunologist and Assistant Professor at LSU (Shreveport) Department of Allergy and Immunology

Classification of ocular allergy (click to enlarge the image).

Alphabet "soup": SAC, PAC, AKC, VKC, GPC (click to enlarge the image).
Allergic Conjunctivitis
- AAC
- SAC
- PAC
Keratoconjunctivitis
- Atopic Keratoconjunctivitis (AKC), atopic dermatitis-related, lower eyelid
- Vernal Keratoconjunctivitis (VKC), upper eyelid. See Vernal Keratoconjunctivitis - NEJM images, 2012.
Giant Papillary Conjunctivitis (GPC), contact lenses-related, upper eyelid
Contact dermatoconjunctivitis
All ocular allergies are characterized by bilateral involvement. Sensitization is necessary for all ocular allergies except for giant papillary conjunctivitis.
Most common type of ocular allergy is allergic conjunctivitis (80-90% of all cases).
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
Allergic conjunctivitis
Allergic conjunctivitis is a relatively benign disease that does not threaten vision. Ocular allergy is estimated to affect 20-25% of the population and the incidence is increasing.
Clinical Manifestations
Allergic conjunctivitis is a disease of young adults (average age of onset 20 years).
As with many allergic diseases, symptoms decrease with age.
50% of patients have a personal or family history of other allergic conditions such as allergic rhinitis, atopic dermatitis, and asthma
Signs and symptoms
Itching, tearing, conjunctival edema, hyperemia, watery discharge, burning, and photophobia, eyelid edema.
Laboratory findings
Allergic conjunctivitis is a clinical diagnosis.

Diagnostic Tests in Allergic Conjunctivitis (of academic interest) (click to enlarge the image).
Some tests of academic interest:
- Conjunctival scrapings show eosinophils in 80%
- Tear film and serum IgE levels are elevated
- Tear film mast cell activity is increased - measured by immunoassay for tryptase (unique to mast cells).
But rubbing by itself can result in a significant increase of tryptase in tears.
Conjunctival provocation test (CPT)
CPT is used to study AC and drug efficacies. Before undergoing a CPT, patients must first be skin tested to determine the appropriate allergen for each patient. The allergen extract is applied bilaterally into the conjunctival sac of the eyes.
At baseline, 2 visits (7 days apart) are used to establish the threshold dose of allergen (visit 1) and reproducibility (visit 2).
CPT is a double-blind, randomized test in which the test drug is applied to one eye and placebo to the other.
Types of allergic conjunctivitis
3 categories
- Acute allergic conjunctivitis (AAC)
- Seasonal allergic conjunctivitis (SAC)
- Perennial allergic conjunctivitis (PAC), less common and less severe than SAC
The main difference between SAC and PAC is the timing of the symptoms. SAC symptoms last a specific season. PAC symptoms last throughout the year.
Acute allergic conjunctivitis (AAC)
Sudden-onset hypersensitivity reaction caused by environmental exposure, for example, such as cat dander.
AAC can be severe and debilitating. However, most cases of AAC are self-limited to 24 hours and do not require long-term treatment.
Seasonal allergic conjunctivitis (SAC)
There are several synonyms for SAC: allergic conjunctivitis, hay-fever conjunctivitis, or allergic rhinoconjunctivitis.
SAC is a milder form of ocular allergy than AAC, typically associated with allergic rhinitis (AR).
SAC is most commonly triggered by ragweed or grass pollens.
SAC has a chronic course that corresponds to pollen seasons: tree pollens in the spring, grass pollens in the summer, and weed pollens in the late summer and fall.
Perennial allergic conjunctivitis (PAC)
PAC is a mild chronic allergic conjunctivitis related to year-round indoor allergens, for example, house dust mite (HDM), animal dander, and molds.
PAC is less common and less severe than SAC.
Pathophysiology
All 3 types result from type I IgE–mediated hypersensitivity, same as other atopic diseases.
Conjunctival scrapings show 2 phases (early and late) of the allergic response, same as other atopic diseases affecting the skin, nose and lungs.
The immediate response to allergens is mediated by mast cells, which are normally present in high concentrations in the conjunctiva.
Allergen-IgE crosslinking causes mast cells to release chemical mediators.
Histamine is the mediator of the early response.
Late response consists of cell influx (eosinophils, basophils, and neutrophils) which usually takes 6-10 hours after allergen challenge.
Eosinophils release leukotriene C4, eosinophilic peroxidase, eosinophilic cationic protein, and histamine into the tear fluid.
Diagnosis
The diagnosis of allergic conjunctivitis is usually clinically apparent in the context of typical history and physical examination findings.
The dominant symptom in AC is itching. The eye appears red. Typically, itch is not reported with dry eye.
Laboratory tests are not usually needed to confirm the clinical diagnosis of AC.
Differential diagnosis
- infectious conjunctivitis
- blepharitis
- dry eye
Allergic conditions are often accompanied by pruritus which is not common in infections.
Management
General measures:
- do not to rub the eyes. Eye rubbing causes mechanical mast cell degranulation.
- artificial tears several times a day
- allergen avoidance
- topical antihistamine eye drops
- cool compresses
-avoidance of contact lenses use -- allergens adhere to contact lens surfaces
Dry eyes or tear film insufficiency are extremely common.
Signs of tear film insufficiency include superficial punctate-keratopathy, reduced tear break-up time, and decreased production of tears as measured by the Schirmer's test.
Oral antihistamines can exacerbate tear film insufficiency through decreased tear production (anticholinergic effect).
Punctal plugs may be helpful and can be placed quickly and painlessly by an ophthalmologist.
Allergen avoidance
SAC:
- limit outdoor exposure
- air conditioning
- car and home windows closed
PAC:
- replacement of old pillows and mattresses
- covers for pillows and mattresses
- frequent washing of beddings
- reducing humidity
- frequent vacuuming and dusting of the home
- remove reservoirs of dust: old carpets, old furniture, old curtains or drapes
- if allergic to animal dander, remove the animal from the home
Immunotherapy
Immunotherapy is effective for treatment of allergic rhinoconjunctivitis
One meta-analysis included 15 studies of immunotherapy in patients with ocular allergy symptoms - 12 studies showed benefit -- decreased ocular symptoms scores and medication use.
Immunotherapy is useful treating ocular symptoms that coexist with allergic rhinitis or asthma but the its role in treating isolated ocular allergy is less clear.
Medications

Medications for Allergic Conjunctivitis (click to enlarge the image).
Medications for AAC
Most cases of AAC are self-limited to 24 hours and do not require long-term treatment.
Over-the-counter topical antihistamine/vasoconstrictor
Over-the-counter topical antihistamine/vasoconstrictor can be used to treat symptoms of short-duration (less than 2 weeks):
- Naphazoline/pheniramine maleate (Naphcon-A®, Opcon-A®, Visine-A®)
- Naphazoline/pheniramine phosphate (Vasocon-A®)
Topical vasoconstrictor (decongestants) work within minutes with a duration of 2 hours. Dosing is QID.
Use for longer than 2 weeks can lead to rebound hyperemia.
Antihistamines
Topical antihistamines are faster-acting than oral anthistimines and have little systemic effects.
The combination of a topical antihistamine and a vasoconstrictor works better than either agent alone.
Frequent attacks of AAC (more than 2 days per month) are treated with a dual-action agent (antihistamine/mast cell stabilizer) such as olopatadine.
Pataday® is used qd, Patanol® is used bid for prevention and qid for acute symptoms.
Other topical antihistamines and/or mast cell stabilizers: azelastine (Optivar®), epinastine (Elestat®), pemirolast (Alamast®), and ketotifen (generic).
Ketotifen bid is generic and over-the-counter.
Dual-acting, Antihistamine and Mast Cell–Stabilizing Drugs
These most commonly prescribed eye drops for allergic eye disease: azelastine, olopatadine, and ketotifen.
Medications for SAC and PAC
5 classes of topical drugs:
1. antihistamines
2. mast cell stabilizers, e.g. cromolyn
3. antihistamine/mast cell stabilizer combinations, e.g. olopatadine, ketotifen
4. steroids
5. non-steroidal anti-inflammatory agents (NSAIDs), e.g. ketorolac
Mnemonic for medications for SAC and PAC: MD VANS
Mast cell stabilizers
Dual-acting: antihistamine/mast cell stabilizer
Vasoconstrictors, not recommended
Antihistamines
NSAIDs, only ketorolac, not recommended
Steroids, only loteprednol, by opthalmologist
The treatment of choice for AC is dual–acting eye drops (antihistamine/mast cell stabilizer).
Treatment for SAC should be started 2 weeks prior to the onset of season which cases symptoms: tree pollens in the spring, grass pollens in the summer, and weed pollens in the late summer and fall.
Dual-action agents (topical antihistamines with mast cell stabilizing properties):
- olapatadine (Patanol®, Pataday®)
- azelastine HCl (Optivar®)
- epinastine (Elestat®)
- pemirolast (Alamast®)
- ketotifen (generic)
Ocular antihistamines (eye drops) (click to enlarge the image).
Mast cell stabilizers:
- cromolyn (generic, Opticrom®)
- lodoxamide (Alomide®)
The onset of action of mast cell stabilizers is slow (5-14 days) and the dosing is QID (inconvenient). Cromolyn cannot be used for acute symptoms.
One study compared cromolyn (4%, 4 times daily) for 2 weeks prior to allergen challenge to a single drop of ketotifen (0.025 percent) used just before the allergen challenge. The single drop of ketotifen was more effective.
Oral antihistamines
Oral antihistamines are less effective than topical olopatadine or topical ketotifen.
All antihistamines dry the ocular surface due to their atropine-like effect which decreases tear production of the lacrimal glands.
Oral antihistamines reach a peak serum levels in 0.5-3 hours depending on the drug but a full effects is after several days of use (similar to cromolyn). Oral antihistamines act much slower than topical antihistamines.
Cetirizine may cause sedation in a subset of patients, despite its categorization as non-sedating.
Topical NSAIDs
In theory, NSAIDs block the cyclooxygenase and inhibit the conversion of arachidonic acid to prostaglandins and thromboxanes.
In practice, NSAIDs are less effective than antihistanmines but more effective than placebo. NSAIDs are not recommended for treatment of allergic conjunctivitis.
Ketorolac is the only topical NSAID approved for itching due to AC.
Patients with AR and AC
Olopatadine can be combined with an intranasal steroid (INS). Fluticasone furoate nasal spray is the only intranasal corticosteroid to reduce the ocular symptoms of seasonal allergic rhinitis consistently, JACI, 2010.
When to refer to an ophthalmologist?
If there is no response to 2-3 weeks of an antihistamine/mast cell stabilizer (olopatadine).
Steroids
Only one topical steroid is currently approved for use in ocular allergy—loteprednol.
Loteprednol 0.2% is Alrex.
Loteprednol 0.5% is Lotemax.
Topical steroids may be considered in refractory patients. Topical steroids can cause serious ocular side effects and should only be used for short "pulse therapy."
Side effects of topical steroids can lead to blindness:
- cataract formation
- elevated intraocular pressure (IOP) and glaucoma
- secondary infections
5% of people respond to steroid eye drop with increased intraocular pressure. Of those with a family history of glaucoma, 20-30% respond with elevated intraocular pressure.
Prednisolone acetate (1 %) and dexamethasone phosphate (0.1 %) have the greatest risk of raising IOP.
"Soft" topical steroids have a much llower risk of increased IOP becase they are inactivated after corneal penetration: Lotemax® (loteprednol), Pred Mild® (prednisolone), FML® (fluorometholone), HMS® (medrysone), and Vexol® (rimexolone).
Atopic Keratoconjunctivitis (AKC)
AKC is a chronic ocular inflammation involving the lower tarsal conjunctiva. VKC affects the upper tarsal conjunctiva. See Vernal Keratoconjunctivitis - NEJM images, 2012.
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
The association between atopic dermatitis and AKC was first described in 1953.
Almost all patients with AKC have atopic dermatitis, and many have asthma. Peak incidence of AKC is 20–50 years of age.
3% of the population is affected by atopic dermatitis. 25% of people with atopic dermatitis have ocular involvement.
Secondary staphylococcal blepharitis is common because of eyelid induration and maceration. Herpetic keratitis occurs in 14-18% of patients.
Keratoconus (noninflammatory progressive thinning of the cornea) occurs in 7-16% of patients.
Treatment of Atopic Keratoconjunctivitis
AKC is a sight-threatening disease.
Topical vasoconstrictor-antihistamine combination may bring transient relief. Dual-acting and mast cell–stabilizing drugs are also recommended.
Topical steroids 8 times per day for 7-10 days are needed to control the symptoms and often lead to an excellent response. Steroid use is transient.
Trichiasis (misdirected eyelashes) must be corrected surgically.
Staphylococcal-associated blepharitis and herpes simplex keratitis requires specific treatments.
Vernal Keratoconjunctivitis (VKC)
VKC is a severe bilateral chronic inflammation of the upper tarsal conjunctiva.
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
VKC is not IgE mediated but occurs most frequently in children with seasonal allergies, asthma, or atopic dermatitis. Males predominate 3:1.
"Vernal" means occurring in spring.
VKC onset is generally before 10 years of age. Without treatment, VKC lasts 2-10 years and usually resolves during puberty. Young men in dry, hot climates (Mediterranean, West Africa) are primarily affected.
VKC signs:
Steroids
Only one topical steroid is currently approved for use in ocular allergy—loteprednol.
Loteprednol 0.2% is Alrex.
Loteprednol 0.5% is Lotemax.
Topical steroids may be considered in refractory patients. Topical steroids can cause serious ocular side effects and should only be used for short "pulse therapy."
Side effects of topical steroids can lead to blindness:
- cataract formation
- elevated intraocular pressure (IOP) and glaucoma
- secondary infections
5% of people respond to steroid eye drop with increased intraocular pressure. Of those with a family history of glaucoma, 20-30% respond with elevated intraocular pressure.
Prednisolone acetate (1 %) and dexamethasone phosphate (0.1 %) have the greatest risk of raising IOP.
"Soft" topical steroids have a much llower risk of increased IOP becase they are inactivated after corneal penetration: Lotemax® (loteprednol), Pred Mild® (prednisolone), FML® (fluorometholone), HMS® (medrysone), and Vexol® (rimexolone).
Atopic Keratoconjunctivitis (AKC)
AKC is a chronic ocular inflammation involving the lower tarsal conjunctiva. VKC affects the upper tarsal conjunctiva. See Vernal Keratoconjunctivitis - NEJM images, 2012.
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
The association between atopic dermatitis and AKC was first described in 1953.
Almost all patients with AKC have atopic dermatitis, and many have asthma. Peak incidence of AKC is 20–50 years of age.
3% of the population is affected by atopic dermatitis. 25% of people with atopic dermatitis have ocular involvement.
Secondary staphylococcal blepharitis is common because of eyelid induration and maceration. Herpetic keratitis occurs in 14-18% of patients.
Keratoconus (noninflammatory progressive thinning of the cornea) occurs in 7-16% of patients.
Treatment of Atopic Keratoconjunctivitis
AKC is a sight-threatening disease.
Topical vasoconstrictor-antihistamine combination may bring transient relief. Dual-acting and mast cell–stabilizing drugs are also recommended.
Topical steroids 8 times per day for 7-10 days are needed to control the symptoms and often lead to an excellent response. Steroid use is transient.
Trichiasis (misdirected eyelashes) must be corrected surgically.
Staphylococcal-associated blepharitis and herpes simplex keratitis requires specific treatments.
Vernal Keratoconjunctivitis (VKC)
VKC is a severe bilateral chronic inflammation of the upper tarsal conjunctiva.
Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
VKC is not IgE mediated but occurs most frequently in children with seasonal allergies, asthma, or atopic dermatitis. Males predominate 3:1.
"Vernal" means occurring in spring.
VKC onset is generally before 10 years of age. Without treatment, VKC lasts 2-10 years and usually resolves during puberty. Young men in dry, hot climates (Mediterranean, West Africa) are primarily affected.
VKC signs:
- Giant papillae occur on the upper tarsal plate and are described as cobblestoning.
- yellow-white points in the limbus (Trantas dots)
- yellow-white points on the conjunctiva (Horner points)
- corneal “shield” ulcers
- Dennie lines (Dennie-Morgan folds)
Shield ulcers are sterile ulcers which occur where cobblestone papillae are rubbing on cornea.
Children with VKC have measurably longer eyelashes (reaction to ocular inflammation).
VKC is chronic and sight-threatening.
Treatment of Vernal Keratoconjunctivitis
VKC is a sight-threatening disease.
Topical steroids 8 times per day for 7-10 days usually relieves symptoms.
High-dose aspirin therapy has been shown effective (2.4 gm daily)
Topical cyclosporin A (Restasis) has also been used in VKC: Cyclosporine eye drops prevent seasonal recurrences of vernal keratoconjunctivitis in a 2-year study (JACI, 2011).
Giant Papillary Conjunctivitis (GPC)
GPC is linked to chronic exposure to foreign bodies, such as contact lenses. GPC is considered an iatrogenic form of allergic eye disease.
Sensitization not necessary in GCP but is required in all other forms of ocular allergy.
GPC is a chronic inflammation that produces giant papillae (1 mm or greater) on the tarsal conjunctiva of the upper eyelids.
Causes of GPC:
- mechanical trauma secondary to contact lenses
- buildup of protein on the surface of the contact lens causes an allergic reaction
Treatment of Giant Papillary Conjunctivitis
Reduction in the wearing time of contact lenses or total discontinuation is required.
“Artificial tears” help to wash away environmental allergens and lens debris ("protein deposits").
Topical mast cell stabilizers are effective in the treatment of GPC and dual-acting drugs may be the best therapy.
Topical steroids are very effective but should be used only for a short period of time, e.g. 4 times per day for 2-4 days.
Contact lens can be resumed but it often requires a change in the type or material of the contact lenses.
Contact dermatoconjunctivitis
Contact dermatoconjunctivitis is a delayed cell-mediated hypersensitivity reaction (type IV), not an IgE antibody–mediated process.
Contact dermatitis involves the eyelids but can also involve the conjunctivae. Contact dermatitis may be caused by contact lens solutions but a multitude of irritants and allergens have been implicated, for example:
- eye drops, anesthetics, antiviral agents, pilocarpine, timolol
- preservatives in ophthalmic solutions (thiomersal, benzalkonium chloride, chlorhexidine, EDTA)
- cosmetics (eye glosses)
- perfumes
- sunscreens
- adhesives (false eyelashes)
Patch testing is the most useful diagnostic tool for contact dermatoconjunctivitis.
The best treatment is avoidance of the offending agent.
Immunologic Diseases of the Eye
Ocular cicatricial pemphigoid
Peripheral ulcerative keratitis
Episcleritis
Scleritis
Uveitis
List of optometric abbrevations
OU, oculus utro (each eye)
OS, oculus sinister (left eye)
OD, oculus dexter (right eye)
SPK, Superficial punctate keratitis
References
Allergic conjunctivitis. M Reza Dana, MD, MPH, MSc, UpToDate, 16.2, 8/2008.
Chapter 88 – Allergic and Immunologic Diseases of the Eye. Neal P. Barney, Frank M. Graziano. Adkinson: Middleton's Allergy: Principles and Practice, 6th ed.
Allergic Conjunctivitis. Presentation Materials. World Allergy Organization.
Pediatric Ocular Inflammation. Immunology and Allergy Clinic of North America. Volume 28, Issue 1, Pages 169-188 (February 2008).
Chapter 146 – Ocular Allergies. Mark Boguniewicz Donald Y.M. Leung. Kliegman: Nelson Textbook of Pediatrics, 18th ed.
Ocular Allergies. Ask the Expert. AAAAI.
Allergic Conjunctivitis. Ask the Expert. AAAAI.
Allergic conjunctivitis. Handbook of Ocular Disease Management.
Ocular Allergy. Curr Opin Allergy Clin Immunol. 2007; 7(5):424-428. Medscape. Medscape
The Pathophysiology of Ocular Allergy: Current Thinking. C Stephen Foster. Allergy, Volume 50 Issue s21, Pages 6 - 9, 2007.
Online Continuing Education: Ocular Allergy. University of Indiana.
Conjunctivitis, Allergic. Parag A Majmudar, MD. eMedicine.
Allergic rhinoconjunctivitis and differential diagnosis of the red eye. Granet, David. Allergy and Asthma Proceedings, Volume 29, Number 6, 11/12 2008 , pp. 565-574(10).
Updates in the treatment of ocular allergies. Journal of Asthma and Allergy, November 2010, Volume 2010:3 Pages 149 - 158 DOI 10.2147/JAA.S13705 (free PDF).
PowerPoint Presentations
Ocular allergy. V. Dimov, M.D., 09/2008.
Allergic Conjunctivitis. World Allergy Congress.
Allergic Conjunctivitis. MCFP.
Eye diseases and the internist. ACP.
Questions
Review Questions: Pediatric Allergy: Principles & Practices, Chapter 56: Allergic and Immunologic Eye Disease.
Patient information
Patient information: Eye Allergies. WebMD.
Ocular Allergies. Clifford W. Bassett, MD, FAAAAI. Allergy & Asthma Advocate: Summer 2007.
Related reading
Allergy season is here :\ on Flickr
Japanese guideline for allergic conjunctival diseases. Allergol Int. 2011 Mar;60(2):191-203.
Vernal Keratoconjunctivitis - NEJM images, 2012.
Eye Drops for allergic conjunctivitis - why would AAAAI include a homeopathic medications in this list? http://buff.ly/1kPCOgn
Published: 09/25/2008
Updated: 02/02/2012
Vernal Keratoconjunctivitis - NEJM images, 2012.
Eye Drops for allergic conjunctivitis - why would AAAAI include a homeopathic medications in this list? http://buff.ly/1kPCOgn
Published: 09/25/2008
Updated: 02/02/2012
Subscribe to:
Posts (Atom)